Neutropenic Fever · What Is It, Causes, Symptoms, Diagnosis, Risk Assessment, Treatment, Prevention, and More
Published: Mar 04, 2025
Author: Jennifer Cheung, RN•
Editor: Antonella Melani, MD•
Editor: Lisa Miklush, PhD, RN, CNS
Illustrator: Abbey Richard
7-day free trial
Go deeper with Osmosis
Osmosis is a learning platform with videos, questions, and AI tools to help you master topics like this.
Watch quick, visual videos
Practice with Qbank-style questions
Use AI to explain, quiz, and review
Study anytime with the mobile app
No credit card · Cancel anytime
What is neutropenic fever?
Neutropenic fever, also known as febrile neutropenia, is the presence of neutropenia accompanied by a fever. Neutropenia refers to a decrease in the concentration of neutrophils in blood. Neutrophils are a type of white blood cell that helps fight infections as part of the immune system.
The Infectious Diseases Society of America defines neutropenia as an absolute neutrophil count (ANC) of less than 1500 cells/mm3. The risk of infection and neutropenic fever increases dramatically with severe neutropenia, which is defined as an absolute neutrophil count (ANC) below 500 cells/mm3. A fever is defined as either a single oral temperature greater or equal to 101o Fahrenheit (38.3o Celsius) or a sustained temperature greater or equal to 100.4o Fahrenheit (38.0o Celsius) or higher for an hour or longer.Learn deeper with Osmosis
Master this topic faster with videos, questions, and AI.
Used by 8M+ healthcare learners.
Start free trial
No credit card · Cancel anytime
Is neutropenic fever dangerous?
Neutropenic fever can be dangerous and is considered a medical emergency, as a severe decrease in the absolute neutrophil count (ANC) compromises the immune system’s ability to fight against opportunistic infections. Morbidity and mortality depend on severity and duration. Fever and neutropenia that last for less than seven days are associated with a more positive prognosis. Conversely, higher risk of infection-related morbidity and mortality is seen in individuals with persistent neutropenia that lasts for more than seven days, or the presence of profound neutropenia with a neutrophil count lower than 100 cells/mm3.
What causes neutropenic fever?
Neutropenic fever is caused by conditions that decrease neutrophil production or increase neutrophil destruction. Some of these conditions include severe active infections such as sepsis, hepatitis, or tuberculosis; bone marrow disorders like aplastic anemia or myelofibrosis; or autoimmune diseases like systemic lupus erythematosus or rheumatoid arthritis. In addition, neutropenic fever may be caused by cancer treatments such as chemotherapy, radiation therapy, and hematopoietic stem cell transplant (HSCT).
Does chemotherapy cause neutropenic fever?
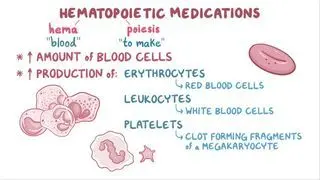
Chemotherapy is one of the most common causes of neutropenic fever, as many chemotherapy medications that destroy tumor cells can also affect the normal production of blood cells, known as hematopoiesis, resulting in myelosuppression and destruction of neutrophils.
To prevent the neutrophil count from decreasing further, chemotherapy dosage may need to be reduced or delayed, which, in turn, can adversely affect the prognosis.
What are the symptoms of neutropenic fever?
In the presence of neutropenia, the usual signs and symptoms of infection may be reduced or absent, and often, fever is the only reliable symptom. Other significant signs and symptoms of infection can include abdominal pain, mucositis of the gastrointestinal tract, and perirectal pain.
Some individuals may develop complications such as severe sepsis or septic shock. Symptoms may include extreme pain, increased heart rate, confusion, shortness of breath, decreased urination, and shivering.How do you diagnose neutropenic fever?
Diagnosis of neutropenic fever involves evaluating individuals for their clinical presentation, including the duration of their fever and any additional symptoms, as well as determining possible sites of infection and causative pathogens. A review of medical history should include recent antibiotic therapy, surgery, invasive procedures, past infections, and potential exposure to infected visitors, pets, plants, or contaminated foods.
Any potential portal of entry for pathogens should be carefully examined, including the skin, mucous membranes, gastrointestinal tract, urinary tract, and any IV catheters or line sites.
Laboratory tests and cultures help determine the causative pathogens. Laboratory tests include a complete blood cell count and differential white cell count to determine the severity of neutropenia. Cultures may involve blood culture sets, a urinalysis, and cultures from other possible sites of infection, such as from the stool, sputum, or nasal swab.
Finally, individuals with neutropenic fever should be examined with chest X-rays, and depending on the clinical presentation, some individuals may need additional imaging studies, such as a CT scan.
How do you assess the risk of medical complications from neutropenic fever?
Individuals diagnosed with neutropenic fever should be evaluated to determine their risk of developing medical complications, such as severe sepsis or septic shock.
The Multinational Association of Supportive Care in Cancer (MASCC) Risk Index is a clinical practice guideline used to identify the risk of medical complications in patients with chemotherapy-induced neutropenia. A MASCC score of 21 points or higher is considered low-risk, whereas a score of 20 or lower is indicative of high-risk for morbidity and mortality.In general, low-risk patients will experience neutropenia for less than 7 days, with no medical complications and stable renal and hepatic functions. A majority of low-risk patients will recover quickly after treatment. Generally, patients with solid tumors are considered low-risk for neutropenic fever.
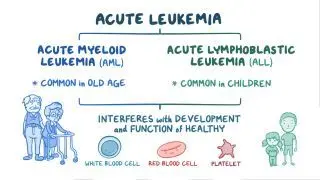
Conversely, high-risk patients may experience profound neutropenia for more than 7 days. These patients may have more sites of infection, such as recent surgery or invasive procedures like biopsies, use of indwelling catheters, or exposure to infectious organisms from family members, food, pets, and travel. High-risk patients often have medical complications like diabetes, chronic lung disease, or malnutrition. Other factors that increase infection risk include a past episode of neutropenic fever and recent treatment with broad-spectrum antibiotics. Generally, people with myeloid and hematologic cancers like leukemia are considered high-risk for neutropenic fever.
How do you treat neutropenic fever?
Treatment begins with an immediate evaluation, risk assessment for complications, and blood cultures to find the causative bacteria. Then, individuals are given broad-spectrum empiric antibiotic therapy. Low-risk patients are commonly given oral antibiotics, while high-risk patients generally get intravenous antibiotics.
Although infection with Gram-positive bacteria is more common, infection with Gram-negative bacteria is associated with higher morbidity and mortality, so using antipseudomonal beta-lactam agents like piperacillin-tazobactam is preferred. Individuals with hypotension or septic shock may require a multidrug approach, combining more than one antibiotic until blood culture results come back.
In cases where fever and neutropenia persist for more than 4–7 days despite empiric antibiotic therapy, a fungal infection can be suspected. Treatment includes initiating empiric antifungal therapy, while CT scans of the chest and serial galactomannan assay results may aid in identifying possible fungal infections and guide further treatment.How do you treat neutropenic fever at home?
Low-risk individuals with neutropenic fever can be treated at home with empiric antibiotic therapy and mandatory close follow-up. Caregivers must practice strict standard precautions. Persistent fever or new signs or symptoms of infection may require admission to the hospital.
How do you prevent neutropenic fever?
Preventing neutropenic fever begins by taking steps to limit exposure to opportunistic pathogens. Measures include daily baths, oral hygiene, routine inspection of the skin and other portals of entry, cleaning and cooking food well, as well as avoiding contact with pets, plants, and visitors with active infections. Additionally, with hospitalized patients, healthcare workers and caregivers should practice standard precautions, including regular hand hygiene and utilizing personal protective equipment, as well as limiting skin breaks or injury by avoiding rectal thermometers, enemas, suppositories, digital rectal examinations, and invasive procedures.
Additional measures can involve giving preventive therapy with colony-stimulating factors that stimulate the bone marrow to increase the production of white blood cells like neutrophils. These agents are administered according to clinical practice guidelines developed by the American Society of Clinical Oncology as a prophylactic treatment in high-risk patients for primary prophylaxis or secondary prophylaxis, or as a combination with antibiotic therapy during active infection with neutropenic fever.
Prophylactic use of antibiotics, antifungal, or antiviral therapy can be beneficial for high-risk patients undergoing procedures that may further compromise the immune system, like hematopoietic stem cell transplantation (HSCT) or induction therapy for leukemia and conditions like high-grade graft-versus-host-disease (GVHD). These individuals may also get screening for herpes simplex virus (HSV), hepatitis, and influenza infections, in order to assess for active or latent infections and initiate prophylactic antivirals.What are the most important facts to know about neutropenic fever?
Neutropenic fever refers to an absolute neutrophil count (ANC) of 500 cells/mm3 or less, accompanied by a temperature greater or equal to 101o Fahrenheit (38.3o Celsius). It is a medical emergency as a severe decrease in neutrophils compromises the immune system’s ability to fight against infection. The most common causes of neutropenic fever are cancer treatments like chemotherapy and hematopoietic stem cell transplant (HSCT). Diagnosis of neutropenic fever involves clinical examination, laboratory tests and cultures, and chest X-rays. Treatment starts with broad-spectrum empiric antibiotic therapy, while empiric antifungal therapy can be considered in cases where fever and neutropenia persist for more than 4–7 days. Preventing neutropenic fever involves limiting exposure to pathogens. Caregivers should practice regular hand hygiene and use personal protective equipment. Other measures include personal hygiene and routine inspection of portals of entry. Additional measures can involve giving preventive therapy with colony-stimulating factors that stimulate the bone marrow.
Related topics



Students say Osmosis is 100% worth it
Because Osmosis saves them time. Lowers stress. And actually helps them remember when it counts.
I used Osmosis to prepare for my first medical school licensing exam! Super helpful and interactive for people who may not do great with just pages of text info!
Cecilia Ruiz
MD student

I have used Osmosis for about four years. Best thing I have ever used for my medical studies.
Sayan Misra
Med student
Osmosis videos are superior because they define simple concepts, tell a story with a clear progression, and provide context.
Jay Pate
Dental student
References
https://www.uptodate.com/contents/risk-assessment-of-adults-with-chemotherapy-induced-neutropenia