

Patient positioning seems simple, but it’s one of the most important ways nurses protect patient safety and comfort. Even small changes like adjusting the bed angle can influence oxygenation, and remaining in one position for too long can lead to skin breakdown. New nurses might also unintentionally make errors, such as raising the head of the bed when a patient is dizzy, which can worsen hypotension.
Proper positioning helps prevent complications, improves the accuracy of assessments, supports procedures, reduces injury risk, and promotes dignity and mobility. Because positioning directly influences physiologic stability and clinical outcomes, nurses must continually assess and adjust positioning throughout their shifts to meet changing needs.
This nursing guide covers seventeen essential patient positions, including what they’re used for and key safety considerations. Whether in the hospital, long-term care, surgical, or emergency settings, choosing the right position can significantly influence patient outcomes.
What is patient positioning?
Patient positioning is the standardized way of placing a patient’s body to protect them from injury and support care or assessment. Positioning describes body orientation, joint alignment, and the configuration of the bed or table. These positions do not describe mobility level, restraint use, or activity orders. Instead, they describe how the body is arranged at a given moment.
Why do patient positions matter in nursing care?
Positioning causes changes in physiology. It directly affects ventilation, venous return, pressure distribution, and access for procedures. Poor positioning increases the risk of aspiration, nerve compression, pressure injuries, and inaccurate assessments. In critical care settings, even small deviations in head or trunk angle can change intracranial pressure or oxygenation. For nurses, positioning is not optional. It’s a continuous intervention that requires ongoing reassessment.
What are the core patient positions every new nurse should know?
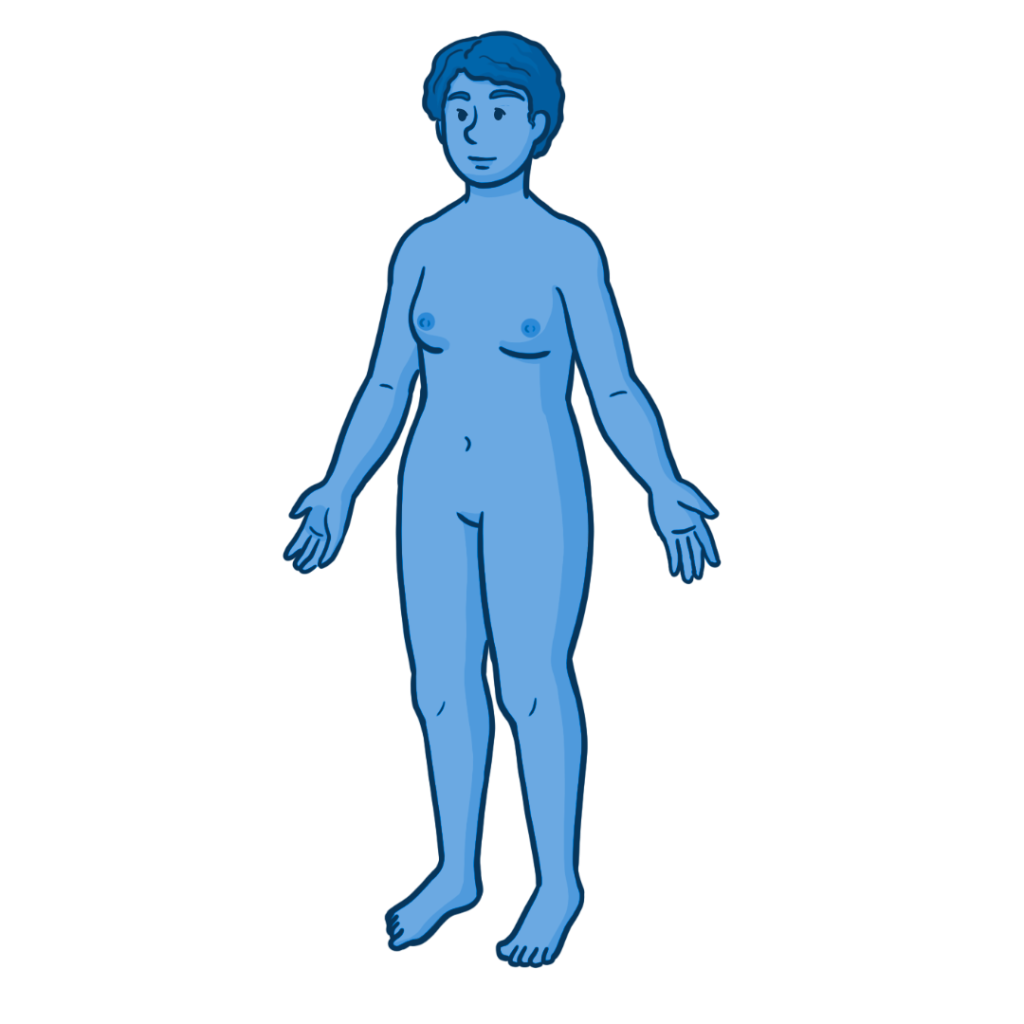
1. Anatomical Position
Description
- The patient stands upright, facing forward, with arms at the sides, palms facing forward.
- Feet are flat, parallel, and slightly apart.
When is the Anatomical position used?
- It serves as a universal anatomical reference for education, documentation, and procedures.
- Ensures that terms such as ‘left arm’ always refer to the body in anatomical position, regardless of the patient’s actual position.
Key Safety Considerations
- Not an actual position, but it helps prevent miscommunication about a patient’s left and right sides.
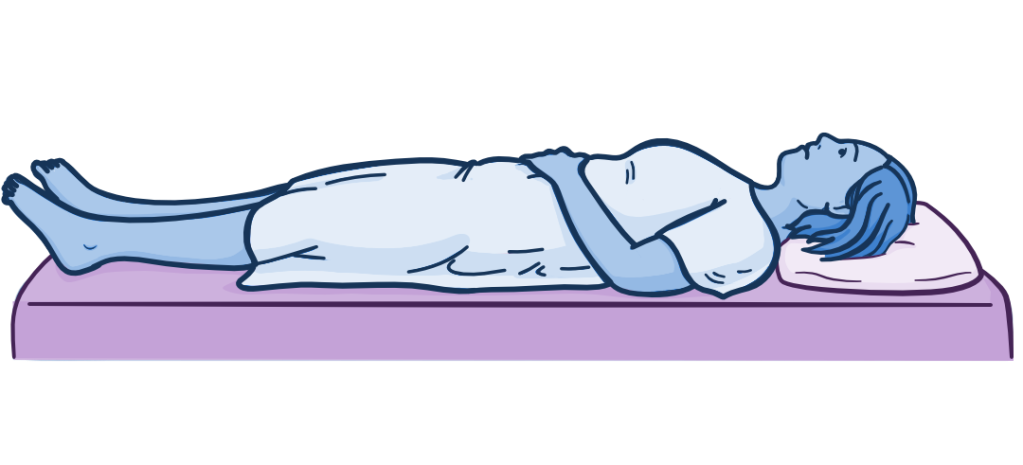
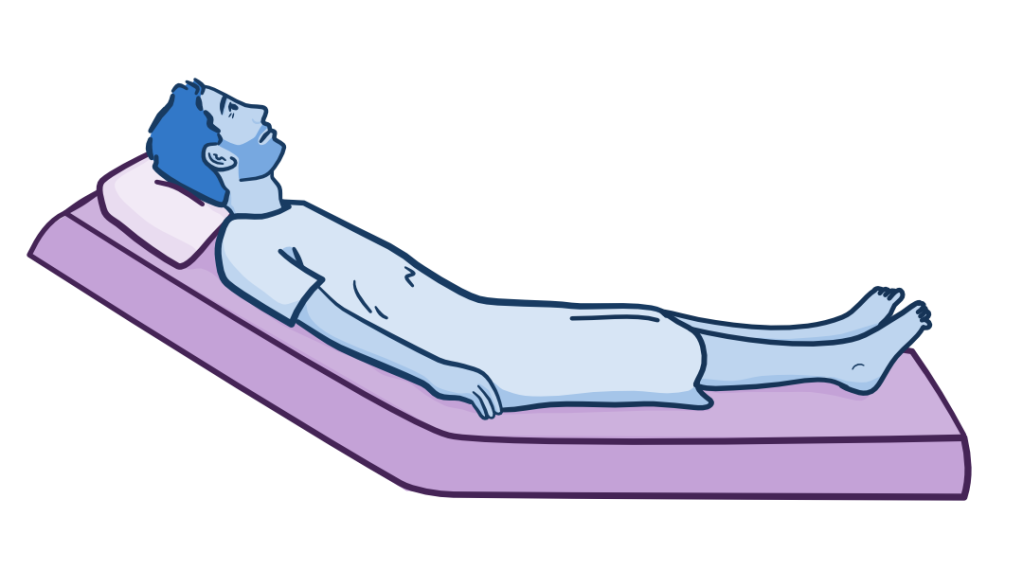
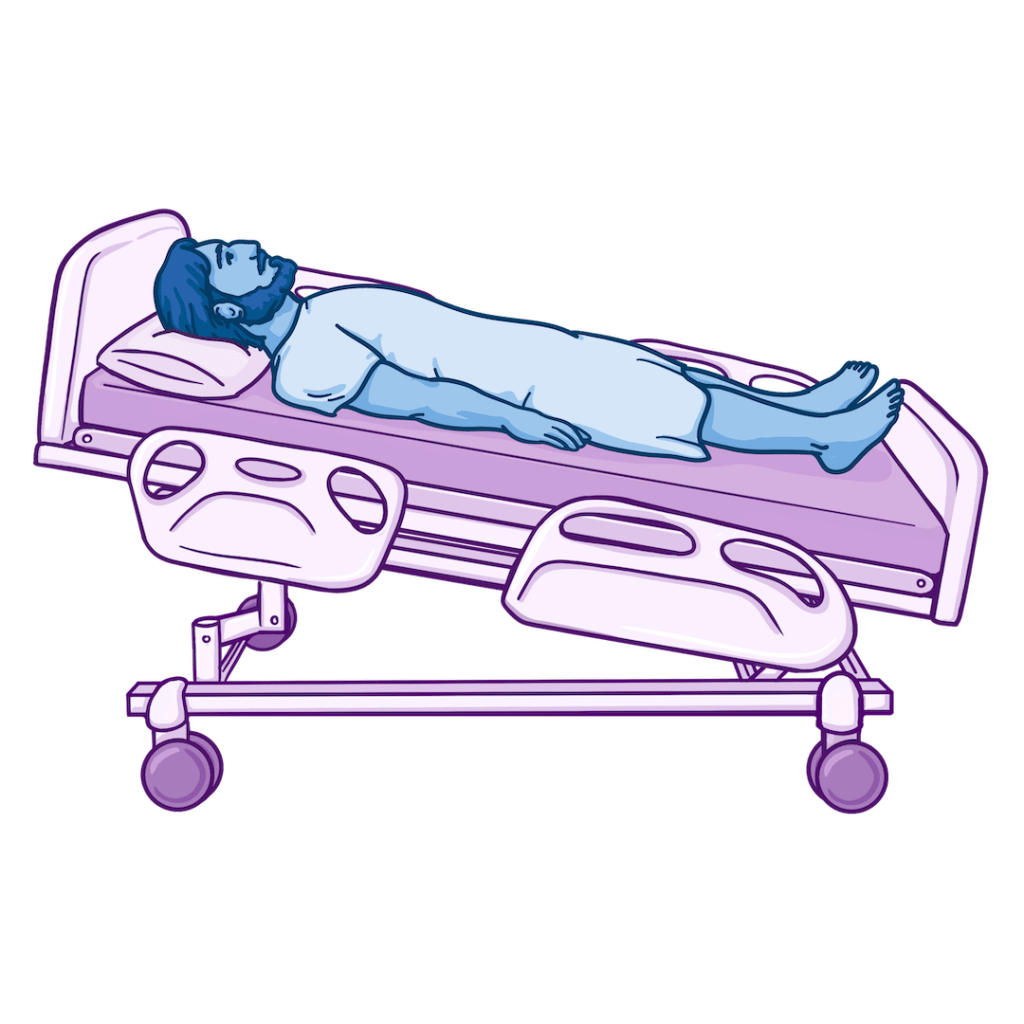
2. Supine Position
Description
- The patient lies flat on their back with their head, shoulders, and hips aligned.
- Legs are extended, and arms rest comfortably at their sides, sometimes with support.
When is the Supine position used?
- Common for exams, imaging, and many procedures
- CPR with a backboard for compressions
- After certain spinal or surgical procedures requiring flat bed rest
- Positioning patients with unstable neck and back injuries in combination with a C-collar
Key Safety Considerations
- Reduces lung expansion and increases risk of aspiration, especially if airway reflexes are impaired.
- It can worsen breathing and discomfort in heart failure.
- Offload pressure on heels, sacrum, elbows, and occiput; reposition frequently.
- Support the lumbar spine and consider pillows under the knees if appropriate.
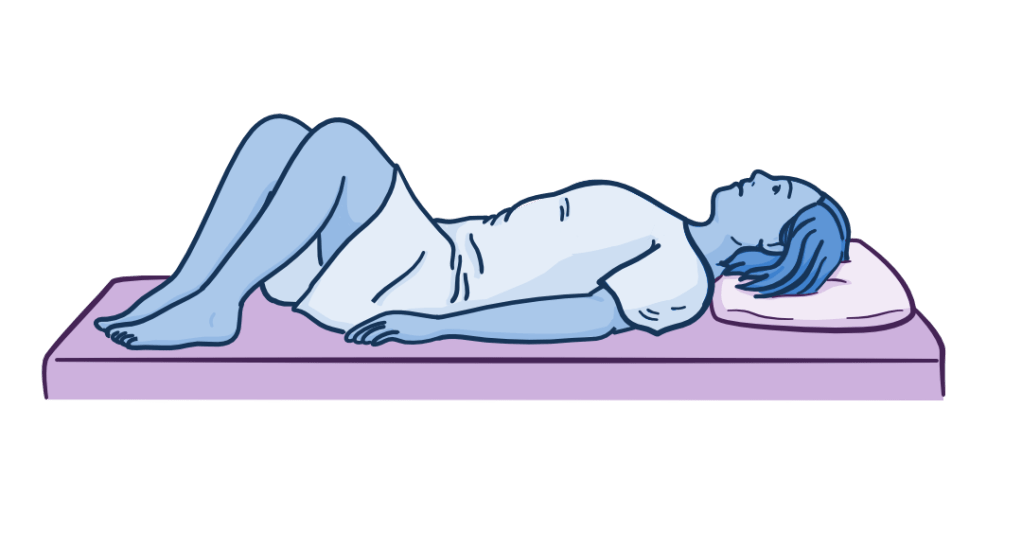
3. Dorsal Recumbent Position
Description
- The patient lies on their back, similar to the supine position, but with knees flexed and feet flat on the bed.
- It improves relaxation of abdominal musculature and is more comfortable for patients with lower back pain than supine positioning.
When is the Dorsal Recumbent position used?
- During abdominal, perineal, and vaginal assessment.
- For urinary catheter insertion and perineal care.
Key Safety Considerations
- Support the knees and lower back.
- Remember to reposition often as this position creates pressure on the feet and might cause hip discomfort.
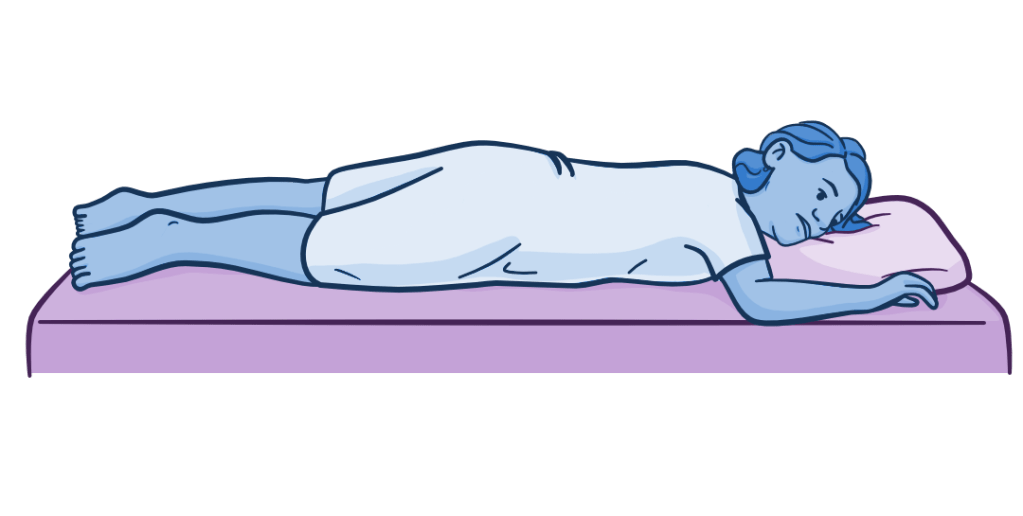
4. Prone Position
Description
- The patient lies on their abdomen with their head turned to one side.
- Arms may be flexed or extended, depending on tolerance.
When is the Prone position used?
- It improves oxygenation and lung expansion.
- Helpful in pressure redistribution or posterior wound care.
- Used in some spinal surgeries.
- In severe acute respiratory distress syndrome (ARDS), intubated and sedated intensive care unit (ICU) patients might be placed in a motorized bed that rotates them slowly into a prone position.
Key Safety Considerations
- Limits airway access, so monitor the airway and any tubing closely.
- Shifts pressure points to the front of the body; use padding to protect the face, breasts, and genitalia.
- This position shouldn’t be used for patients with increased abdominal pressure, hemodynamic instability, high intracranial pressure (ICP), or wounds to the face or front of the body.
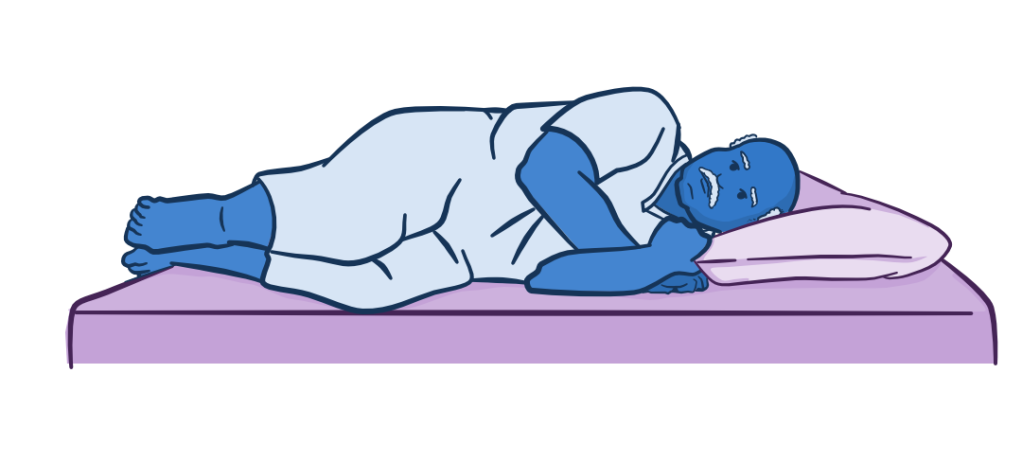
5. Lateral (Side-Lying) Position
Description
- The patient lies on either side with hips and knees slightly flexed.
- Pillows support the head, back, and between the knees.
When is the Lateral (Side-Lying) position used?
- This position is great for patient comfort and pressure relief.
- Aids in secretion management to reduce aspiration risk.
Key Safety Considerations
- Avoid this after shoulder, back, rib, or hip injuries or surgeries.
- Make sure the spine is aligned. and support the knees, hips, and elbows with pillows or foam wedges.
- Switch sides regularly.
- For patients with severe cardiovascular or respiratory instability, this position can cause acute decompensation.

6. Sims Position
Description
- The patient lies in the left lateral position with the right hip and knee flexed.
- Alternate names: Semi-prone, Left-lateral
When is the Sims position used?
- For most rectal procedures and exams, including colonoscopies and enema administration.
- A common pregnancy position to reduce compression of the vena cava, improve comfort, and help with fetal rotation.
Key Safety Considerations
- Like side-lying, this position can cause pressure and injury to the left shoulder and to the parts of the patient’s body in contact with the bed if in this position for too long.
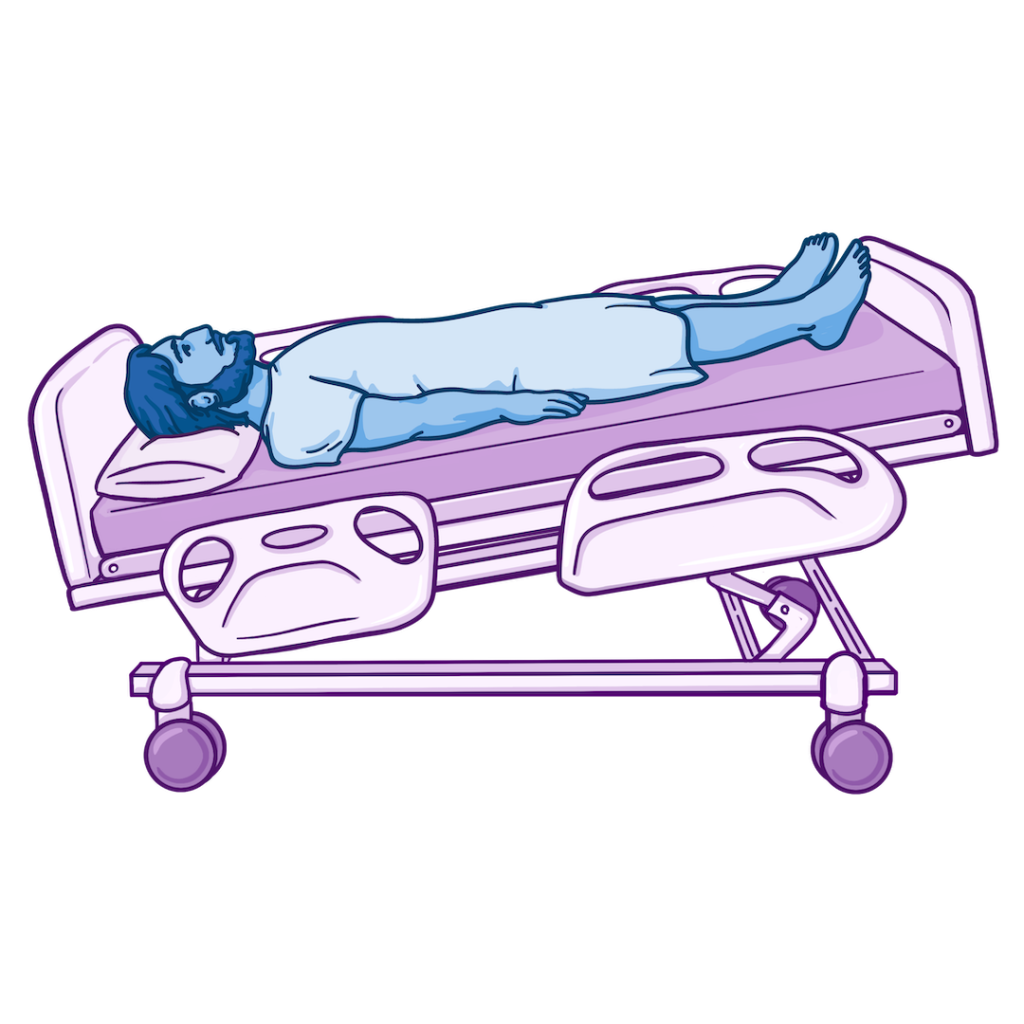
7. Low Fowler Position
Description
- The patient lies supine (on their back) with the head of bed elevated 15–30 degrees.
When is the Low Fowler position used?
- Early postoperative recovery.
- It provides mild respiratory support compared to lying flat.
- This is a common position for patient comfort.
Key Safety Considerations
- Avoid elevating the head of the bed for patients who are dizzy or have low blood pressure.
- Placing pillows under the knees and shifting hips with a wedge or pillow can help improve overall comfort and prevent patients from sliding down in bed.
- Check and reposition immobile patients frequently.

8. Semi-Fowler Position
Description
- The patient lies supine (on their back) with the head of bed elevated 30–45 degrees.
When is the Semi-Fowler position used?
- To improve respiratory comfort
- To help prevent aspiration during enteral feedings
- For improved drainage for nasogastric (NG) tubes
Key Safety Considerations
- Being positioned higher in bed increases the risk of sacral shearing.
- Prevent sliding by supporting the legs under the knees and offload weight from the coccyx with a foam wedge or pillow.
- Check for pressure injuries and reposition frequently, especially with immobile patients.
9. High Fowler Position
Description
- The patient lies supine (on their back) with the head of the bed elevated 60–90 degrees.
When is the High Fowler position used?
- For severe dyspnea or respiratory distress.
- With oral and enteral feedings to prevent aspiration and reflux.
Key Safety Considerations
- May worsen hypotension and fatigue.
- Monitor hemodynamic status, especially when changing positions or raising the head of bed.
- Implement fall precautions and consider using side rails and fall alarms.

10. Orthopneic Position
Description
- The patient sits upright and leans forward with arms supported on a table or pillows.
- Maximizes chest expansion by decreasing the work to breathe.
When is the Orthopneic position used?
- For severe shortness of breath, especially orthopnea that occurs when laying down.
- During COPD and exacerbations of heart failure.
Key Safety Considerations
- Can be tiring; monitor for fatigue and hypotension.
- Ensure the surface the patient is leaning on is locked and stable.
- Place the pulse oximeter on the ear or nose rather than the hands, which may have reduced perfusion.

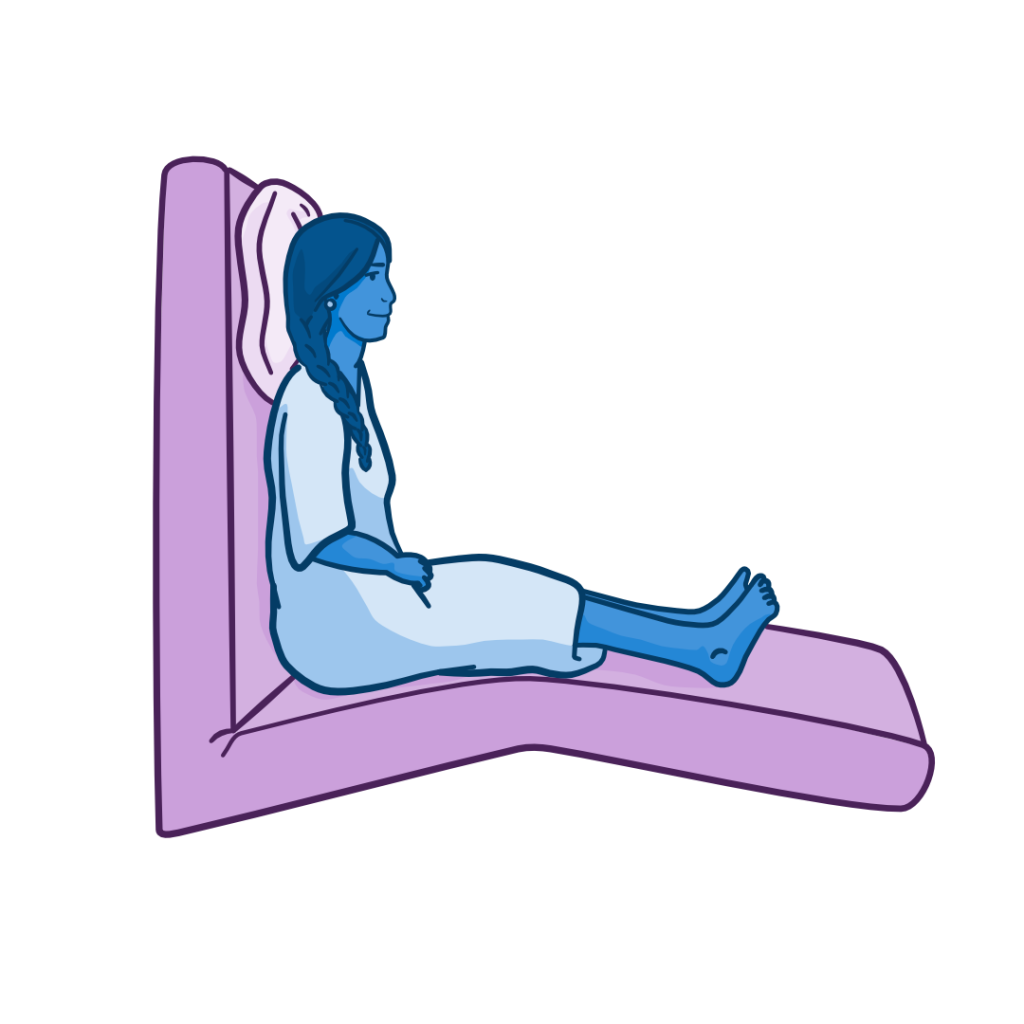
11. Sitting or Upright Position
Description
- The patient sits with feet supported; torso is vertical.
When is the Sitting or Upright position used?
- Some neurological and respiratory assessments.
- Common during patient history and assessments.
- For lab draws and IV fluid administration.
- For oral and enteral feedings.
Key Safety Considerations
- Contraindicated for orthostatic hypotension.
- If the patient was previously unable to tolerate sitting, gradually change to this position and monitor their heart rate, blood pressure, and respiration.
Specialized and Procedural Positions

12. Lithotomy Position
Description
- The patient lies supine with hips flexed 80-90 degrees, knees sharply bent, and legs supported in stirrups.
When is the Lithotomy position used?
- Gynecologic, obstetric, urologic, and colorectal procedures.
Key Safety Considerations
- It can cause nerve compression and circulatory compromise.
- Raise and lower legs simultaneously.
- Assess neurovascular status frequently.
13. Trendelenburg Position
Description
- The patient lies supine with the head lower than the feet.
When is the Trendelenburg position used?
- During selected surgical exposures and central line placement support.
Key Safety Considerations
- Increases intracranial pressure and reduces lung capacity.
- It can cause brachial plexus injuries if shoulder braces are used during procedures.
- Limit duration; monitor respiratory and hemodynamic tolerance.
- For hypotension and hypovolemic shock, use a modified Trendelenburg or passive leg raise, or Shock position, instead, lifting the legs only slightly above the level of the head and chest.
- Typically protocol-driven (e.g., ARDSnet criteria) and requires a trained team due to high risk (tube dislodgement, pressure injuries).
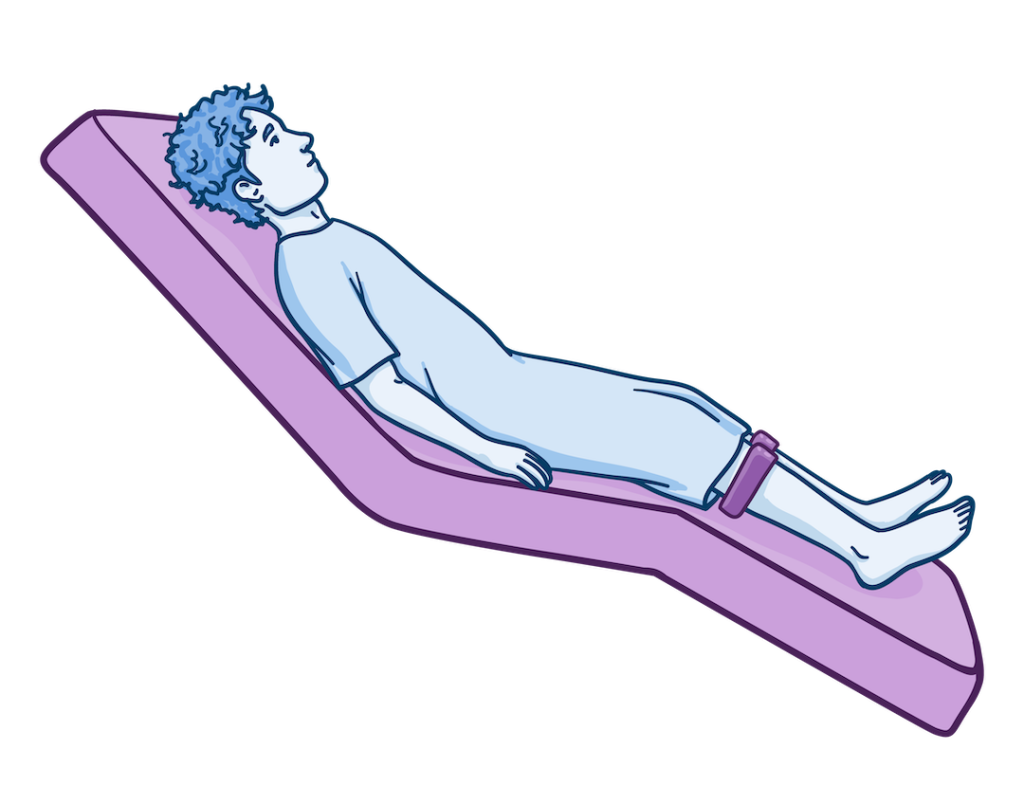
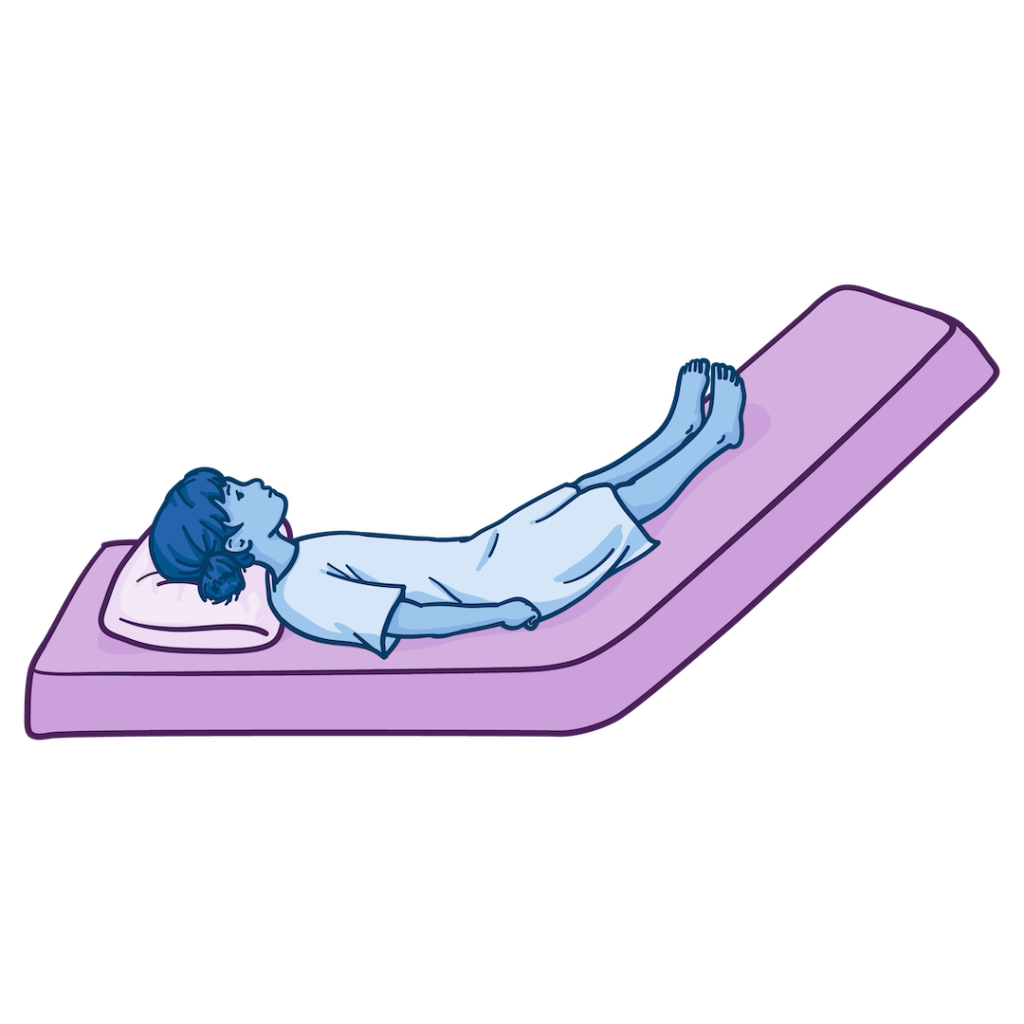
14. Reverse Trendelenburg Position
Description
- The patient lies supine with head elevated above feet; the patient’s body remains straight, and the entire bed frame is tilted rather than just the head of the bed.
When is the Reverse Trendelenburg Position used?
- During upper abdominal procedures.
- For reflux reduction.
- To reduce intracranial pressure.
- As an alternative to the Fowler position, when needing neutral spinal alignment.
Key Safety Considerations
- Secure the patient to prevent sliding using the footboard or positioning aids.
- Monitor pressure points.
- Monitor for hypotension and dizziness with position changes.

15. Knee-Chest Position
Description
- The patient rests on their knees and chest with the hips elevated.
When is the Knee-Chest position used?
- Rectal or sigmoidoscopy assessments or procedures.
- Reducing the risk of umbilical cord prolapse or fetal malpresentation during labor.
Key Safety Considerations
- It can cause respiratory compromise and hemodynamic instability.
- Monitor for discomfort and reduced circulation, particularly in the legs.
- Use only for brief periods.
- Provide privacy and support.
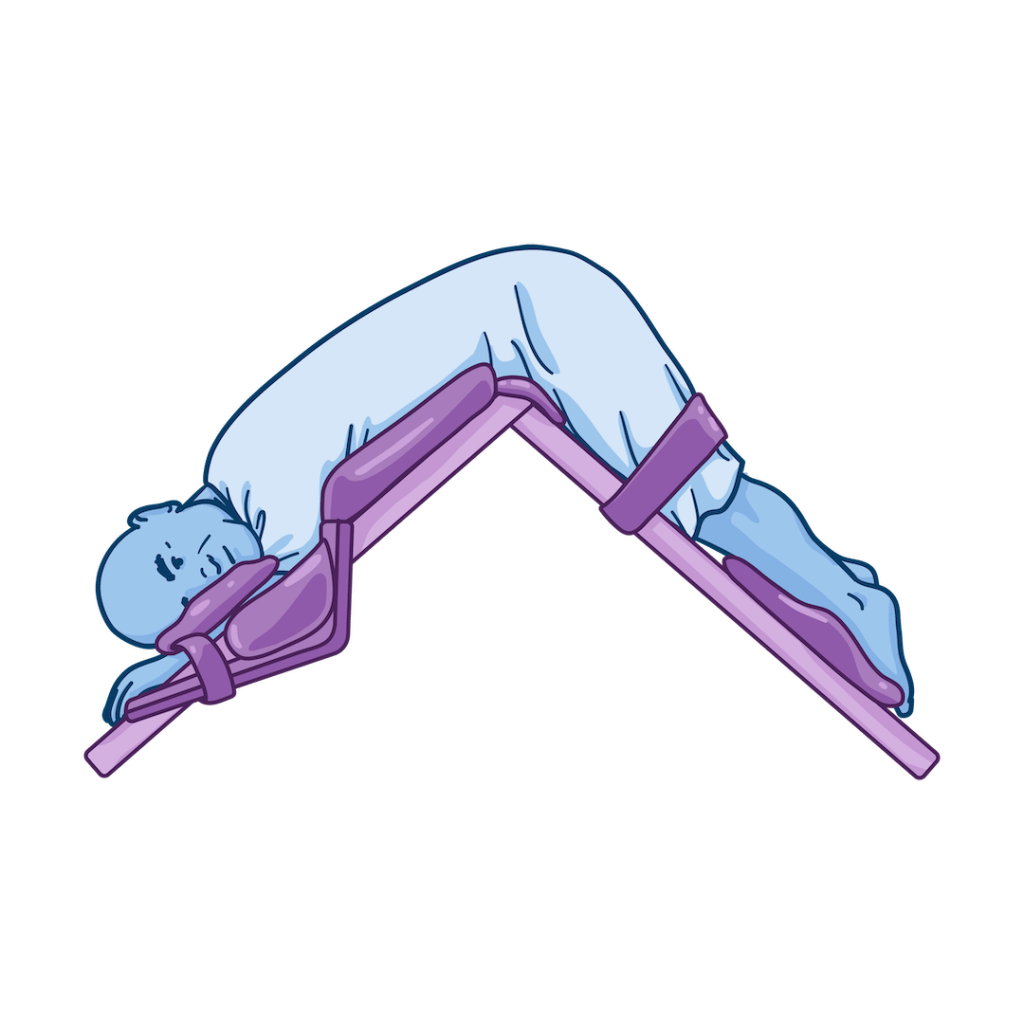
16. Jackknife (Kraske) Position
Description
- A specialized surgical position where the patient lies prone with hips flexed and elevated to create an inverted V with the body.
- The operating table bends at the patient’s hips to achieve this angle.
When is the Jackknife (Kraske) position used?
- For rectal and sacral assessment and procedures.
- In posterior spinal procedures involving the lower spine.
Key Safety Considerations
- Increases pressure injury risk, so be sure to pad bony prominences and pressure points, and check and reposition the patient frequently.
- Restricts chest expansion, so ensure adequate ventilation support.
- Can cause hypotension; monitor blood pressure and change positions slowly.
17. Lloyd-Davies (Modified Lithotomy) Position
Description
- The patient lies supine with hips flexed 30-45 degrees (less than standard lithotomy); knees flexed, legs supported in stirrups or leg holders.
- Alternate Name: Modified lithotomy position.
When is the Lloyd-Davies (Modified Lithotomy) position used?
- During colorectal surgery, gynecologic procedures, urologic procedures, and surgeries requiring abdominal and perineal access.
Key Safety Considerations
- This can cause nerve compression and compartment syndrome risk.
- Monitor for hypotension when returning legs to the supine position.
- Do frequent neurovascular and skin assessments.
- Pad contact points with leg holders.
Patient Positioning for Respiratory, Cardiac, and Neurologic Care
Position changes alter ventilation-perfusion, venous return, and intracranial pressure. Elevating the head supports oxygenation. Prone positioning under protocol improves oxygenation in selected mechanically ventilated patients with ARDS. Neutral head alignment supports cerebral venous drainage and may help limit increases in intracranial pressure. Raising the legs can temporarily help in hypovolemic shock.
Patient Positioning for Imaging, Procedures, and Diagnostics
Diagnostic positioning supports accuracy and safety. Nurses prepare patients, maintain alignment, monitor tolerance, and manage devices during X-ray, CT, MRI, lumbar puncture, endoscopy, and catheterization. Positioning follows institutional protocols and imaging requirements.
Patient Safety, Skin Integrity, Pressure Injury Prevention, and Comfort
Pressure injuries form over bony prominences during sustained positioning. Repositioning schedules, support surfaces, and careful padding reduces risk. High-risk areas vary by position and patient condition, and repositioning should be individualized based on risk assessment findings and support surfaces used. Comfort positioning differs from therapeutic positioning. Nurses must identify the intended clinical goal before repositioning.
Special Populations and Positioning Modifications
Patients who are pregnant require uterine displacement, typically with a left lateral tilt, to avoid vena cava compression. Patients with obesity need additional support and careful airway planning. Pediatric patients require size-appropriate alignment. Unconscious or sedated patients need continuous airway and skin monitoring. Spinal precautions require strict neutral alignment.
Patient Positioning as Continuous Care
Patient positioning is a fundamental clinical skill that directly impacts safety, physiology, and outcomes. From basic alignment in supine to specialized surgical positions, each choice carries specific benefits and risks that require clinical judgment and ongoing reassessment. By understanding when and how to use these 17 positions and consistently prioritizing pressure injury prevention, airway protection, and hemodynamic stability, nurses can reduce complications, support procedures, and improve patient comfort. Ultimately, effective positioning is not a one-time task, but a continuous, evidence-based intervention integrated into every aspect of patient care.
Patient Position Quick Reference Chart
| Position | Primary Uses | Key Nursing Considerations |
| Supine | Assessment, recovery | Aspiration risk |
| Prone | Respiratory care | Airway monitoring |
| Fowler | Feeding, breathing | Shear prevention |
| Lateral | Pressure relief | Alignment |
| Lithotomy | Procedures | Nerve protection |
| Trendelenburg | Surgical access | Intracranial effects |

Frequently Asked Questions: Patient Positions
What are patient positions in nursing care?
Patient positions describe standardized body placements used by nurses to support assessment, comfort, safety, and procedures.
Why is Fowler position used so often?
The Fowler position supports lung expansion and reduces the risk of aspiration during feeding and recovery. It’s also a comfortable resting position.
When is prone positioning used in nursing?
- Prone positioning is used under protocol for severe respiratory failure and posterior body access.
What is the safest position for an unconscious patient?
- The lateral position helps protect the airway in unconscious patients when spinal injury is not suspected.
Is Trendelenburg still used in nursing care?
- The Trendelenburg position is used selectively due to respiratory and intracranial effects.
How often should nurses reposition patients?
- Repositioning schedules depend on individualized risk levels but often occur at least every two hours.
What position helps reduce aspiration risk?
- Semi-Fowler, high Fowler, or lateral positioning reduces the risk of aspiration.
Are patient positions within the nursing scope of practice?
- Patient positioning is a core nursing responsibility within the nursing scope of practice.
Key Takeaways
- Patient positions guide nursing assessment, safety, and outcomes.
- Each position affects physiology, access, and comfort differently.
- Nursing responsibility includes alignment, monitoring, and reassessment.
- Positioning choices change as the patient’s condition changes.
References
- Harding, M. M., Kwong, J., Hagler, D., & Reinisch, C. (2023). Lewis’s medical-surgical nursing (12th ed.). Elsevier.
- Knight, D. J. W., & Mahajan, R. P. (2004). Patient positioning in anesthesia. Continuing Education in Anesthesia, Critical Care & Pain, 4(5), 160–163. https://doi.org/10.1093/bjaceaccp/mkh044
- Potter, P. A., Perry, A. G., Stockert, P. A., Hall, A. M., & Ostendorf, W. R. (2023). Fundamentals of nursing (11th ed.). Elsevier.

Try Osmosis from Elsevier today! Get your free trial to find out why millions of clinicians and caregivers love learning by Osmosis.
Leave a Reply