Chronic obstructive pulmonary disease (COPD): Nursing process (ADPIE)
Notes
| CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
James Robyn is a 67-year-old male client who was brought to the emergency department, or ED, with a 3-day history of exertional breathlessness, wheezing, fatigue, and a worsening productive cough.
He states he has been having increased difficulty with normal day to day activities such as eating, talking and going up the stairs.
He has a history of cigarette smoking, two packs per day, since he was 25 years old.
However, he quit smoking a year ago after being diagnosed with chronic obstructive pulmonary disease, or COPD.
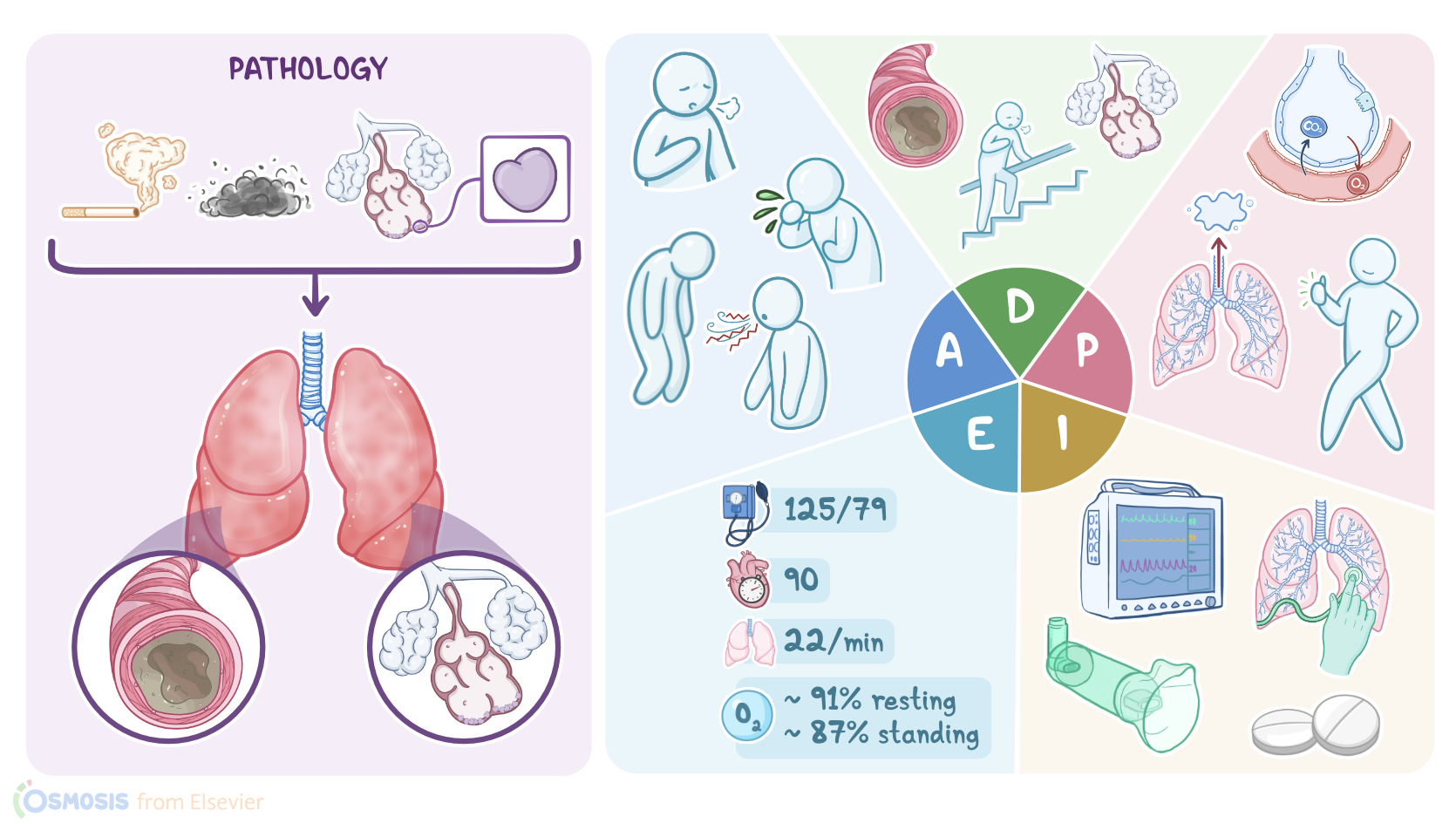
COPD, or chronic obstructive pulmonary disease, is a type of lung disease where chronic inflammation causes damage to the lungs and obstructs airflow.
It’s usually caused by inhalation of toxic substances, like tobacco smoke, or occupational pollutants like dust and silica.
In some people an autosomal dominant disorder called alpha-1 antitrypsin deficiency results in breakdown of the lung parenchyma by an enzyme called elastase.
COPD is characterized by long-term inflammation of the bronchial tubes, referred to as chronic bronchitis, and alveolar destruction, referred to as emphysema.
Most people diagnosed with COPD have elements of both chronic bronchitis and emphysema.
Chronic inflammation of the bronchial tubes in COPD causes a hypersecretion of mucus by the respiratory goblet cells.
The mucus then forms a plug that obstructs the airways causing air trapping, and it also causes chronic productive cough.
Obstruction of the bronchi can also cause exertional dyspnea, which can progress to resting dyspnea, fatigue, wheezing and chest tightness.
Destruction of the alveolar sacs impairs gas exchange, resulting in hypoxemia and hypercapnia.
Loss of elastic recoil causes collapse of the airways during exhalation, trapping the air and dilating the airspaces.
To make breathing easier, they often use the tripod position, where they sit up and lean forward with their hands on their knees.
They may use pursed lip breathing to prolong expiration and produce positive end-expiratory pressure, or PEEP, which allows them to breathe out as much air as possible.
Because this breathing technique requires use of accessory breathing muscles, they will expend a lot of energy just to breathe.
Air trapping also leads to an increased anteroposterior diameter of the chest, sometimes called a barrel chest.
Chronic hypoxemia can result in cyanosis, a bluish discoloration of the lips or fingertips.
It causes constriction of the pulmonary vessels and pulmonary hypertension.
This increases the workload on the right side of the heart, leading to right sided heart failure, or cor pulmonale.
Diagnosis of COPD is based on the client history, physical examination, and pulmonary function tests, or PFTs, to evaluate the degree of airway limitation.
The forced expiratory volume in one second, or FEV1, and the vital capacity, or FVC, are measured after the client is given a bronchodilator such as albuterol.
A FEV1/FVC ratio less than 70% indicates airway obstruction.
Since COPD is an irreversible disease, giving a bronchodilator does not change the person’s PFTs too much.
Finally, alpha-1 antitrypsin deficiency screening may also be done.
Long-term management for stable COPD includes smoking cessation and the avoidance of other triggers such as pollution and allergens.
Influenza and pneumococcal vaccines should be administered to decrease the risk of respiratory infections.
Although COPD is an irreversible disease, bronchodilators can help ease symptoms, and corticosteroids can decrease inflammation in the lungs.
Supplemental oxygen may be needed to maintain an oxygen saturation between 88 to 92 percent.
For these clients, the goal is not 100 percent saturation because hypoxemia is the main stimulus for their respiratory drive.
Finally, since these individuals expend much of their energy on simply breathing, dietary adjustments may be needed to maintain weight and muscle mass.
An exacerbation, or a sustained deterioration of their respiratory symptoms beyond their normal day to day variability, may manifest by increased dyspnea, cough, sputum production, and fatigue.
Increased wheezing may be noted and increased hypoxia may result in confusion or decreased level of consciousness.
Arterial blood gases, or ABGs, may show decreased PaO2, increased PaCO2, increased HCO3-, and decreased pH.
Okay, let’s get back to our client Mr. Robyn.
Since presenting to the ED, he has been admitted to the pulmonary ward for treatment of an acute exacerbation of COPD.
You have been assigned to his care.
After entering his room, you introduce yourself, wash your hands, and confirm his identity.
Mr. Robyn is sitting up on the side of his bed leaning over his bedside table in a tripod position.
You begin your assessment of Mr. Robyn by asking him how he is feeling today.
He states he is feeling short of breath and very tired.
You notice that he struggles to complete full sentences because he has to stop to breathe.
You notice nasal flaring and he is pursing his lips during expiration.
He states that he has had worsening respiratory symptoms for about a week including breathlessness when doing activities such as getting up to go to the bathroom, talking, and eating.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Update on Clinical Aspects of Chronic Obstructive Pulmonary Disease" N Engl J Med (2019)
- "The etiologic origins for chronic obstructive pulmonary disease" Int J Chron Obstruct Pulmon Dis (2019)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations" Clin Chest Med (2020)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)