Anemia - Iron-deficiency: Nursing
Anemia - Iron-deficiency: Nursing
Watch later
Watch later
Notes
| ANEMIA - IRON DEFICIENCY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Iron deficiency anemia is a common condition that occurs when there are decreased iron stores in the body, which is essential for the production of hemoglobin in red blood cells, or RBCs for short.
Now, let’s quickly discuss the physiology of RBC production, or erythropoiesis. This process takes place in the bone marrow, where a stem cell differentiates into an erythroblast, which starts synthesizing hemoglobin, which is a protein that’s able to bind and carry oxygen. Erythroblasts lose their nucleus and differentiate into immature RBCs, called reticulocytes. These immature cells are released from the bone marrow into the bloodstream, to ultimately become mature RBCs, called erythrocytes. Now, RBCs have a limited lifespan of 120 days, so they require continuous replacement through erythropoiesis.
To do so, the body needs important vitamins and minerals, including iron, which is an essential component of hemoglobin. Now, iron is primarily obtained from a balanced diet that includes all types of foods. Once ingested, food passes through the gastrointestinal tract, where nutrients are slowly absorbed. Some nutrients, such as iron, are best absorbed in acidic environments like the proximal duodenum, where gastric acid lowers the pH, in order to absorb iron into the circulation.
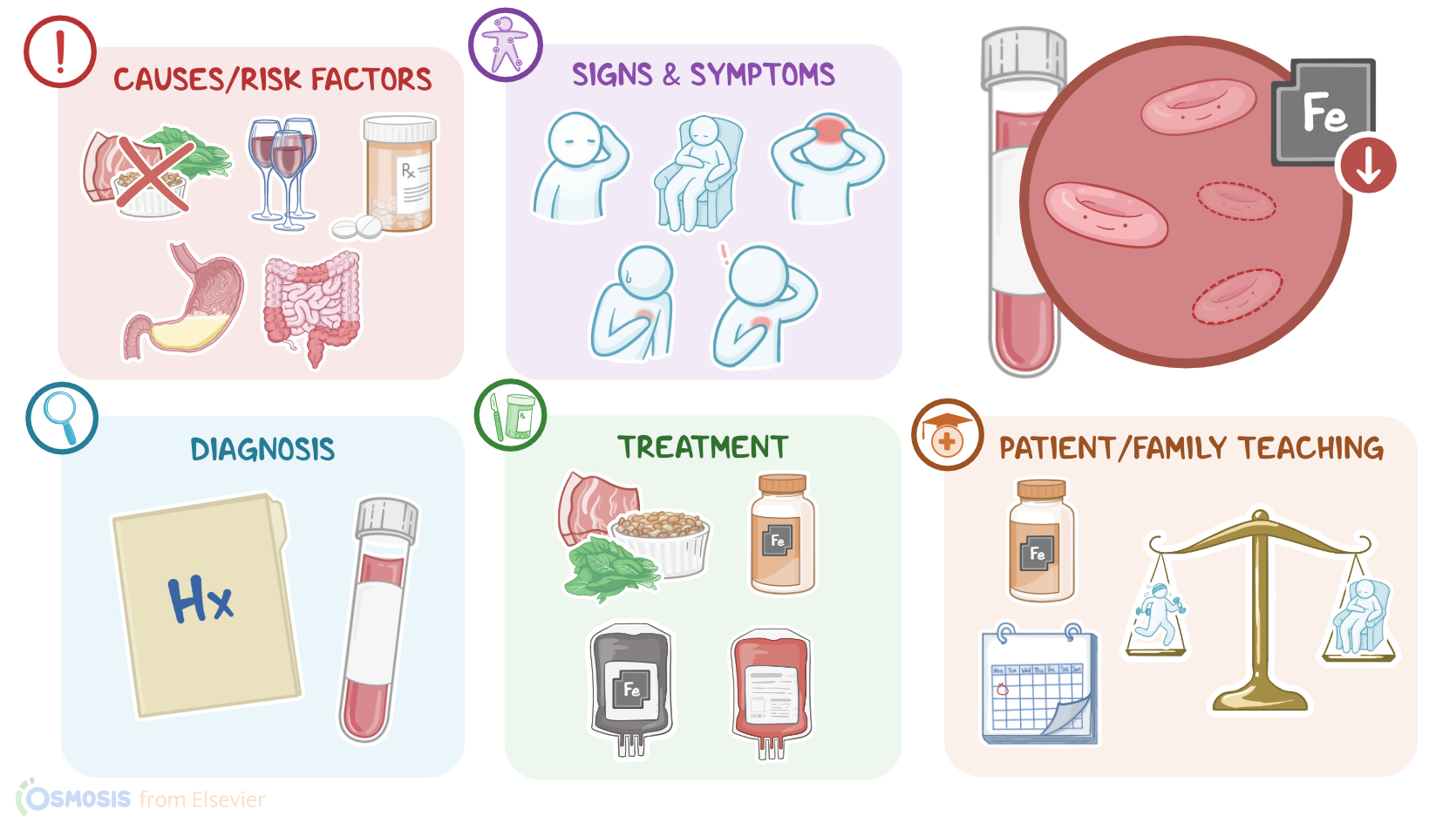
Alright, now iron deficiency anemia can be caused by decreased dietary intake, decreased gastrointestinal absorption, increased body demand, or increased loss. The most common cause of iron deficiency is a decreased intake of iron-rich foods, such as red meat, beans, and leafy greens; risk factors include poor nutritional status from practicing strict diets, chronic alcohol use, and experiencing homelessness, abuse, or neglect.
On the other hand, decreased gastrointestinal absorption of iron can occur due to decreased stomach acid production; risk factors include taking certain medications, such as proton pump inhibitors like omeprazole or H2 blockers like cimetidine; as well as undergoing a gastrectomy, where a part of the stomach is surgically removed. Decreased absorption can also occur due to inflammation of the gastrointestinal tract; risk factors include conditions like inflammatory bowel disease or celiac disease.
Next, increased body demand for iron can occur in children due to rapid growth; as well as during pregnancy and lactation.
Finally, increased iron loss occurs in clients with acute hemorrhage or chronic slow bleeding; or increased hemolysis or destruction of RBCs. Risk factors include trauma, frequent or heavy menstruation, bleeding gastric ulcers, and colorectal cancer; as well as increased autoimmune hemolytic anemia, adverse drug reactions, or even increased destruction by the spleen.
Alright, so the pathology of iron deficiency anemia develops when there is a lack of sufficient iron stores needed to sustain normal hemoglobin production. As a result, there’s not enough hemoglobin to fill a normal-sized RBC, so the bone marrow starts producing microcytic, or smaller, cells that contain less hemoglobin, in order to try to sustain erythropoiesis. These cells also appear paler under the microscope, so they’re also called hypochromic. Some clients may also develop poikilocytes, which are abnormally shaped RBCs that appear flat, elongated, or teardrop-shaped, and may have pointy projections. Lastly, clients may develop anisocytosis, meaning that they have unequally sized RBCs.
The general clinical manifestations of iron deficiency anemia include pallor, weakness, fatigue, and reduced exercise tolerance, as well as headaches, dizziness, and tachycardia. In severe cases, clients with iron deficiency anemia may have decreased oxygen saturation, chest pain, an irregular heartbeat, or systolic heart murmurs.
In addition, clients may also experience a sore tongue with glossitis, and angular cheilitis or fissures around the corners of the mouth, as well as koilonychia or brittle, spoon-shaped nails. Lastly, some clients with iron deficiency anemia may experience pica, where they may crave and eat non-food substances, such as clay or dirt.
Diagnosis of iron deficiency anemia begins with the client’s history and physical assessment, followed by blood tests. These include a complete blood count or CBC, which reveals a decrease in RBC count and hemoglobin. In addition, the reticulocyte count may vary depending on the cause; so it will most often decrease with iron deficiency, but in certain cases it may increase as a compensatory mechanism, such as with hemolysis, as well as in early phases after iron repletion, or when the client is recovering from a hemorrhage.
Key Takeaways
Iron deficiency anemia (IDA) is a condition in which the body is unable to produce sufficient hemoglobin in the red blood cells, due to an inadequate amount of iron in the body. Hemoglobin in the red blood cells is responsible for carrying oxygen throughout the body, so without enough of it, the body doesn't get the oxygen it needs. People with IDA present with symptoms like fatigue, weakness, shortness of breath, and difficulty concentrating. It can also lead to more serious conditions like developmental delay in children, heart failure, and organ damage.
There are several reasons why someone might develop IDA. The most common cause is simply not getting enough iron in your diet. Other causes include bleeding (either internally or externally), chronic illness, and during states in which the body's iron demands are increased such as pregnancy. IDA is characterized by microcytic and hypochromic red blood cells on the peripheral blood smear.