Arrhythmias - Premature ventricular contractions (PVCs): Nursing
1,004views
Notes
| ARRHYTHMIAS - PREMATURE VENTRICULAR CONTRACTIONS (PVCs) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
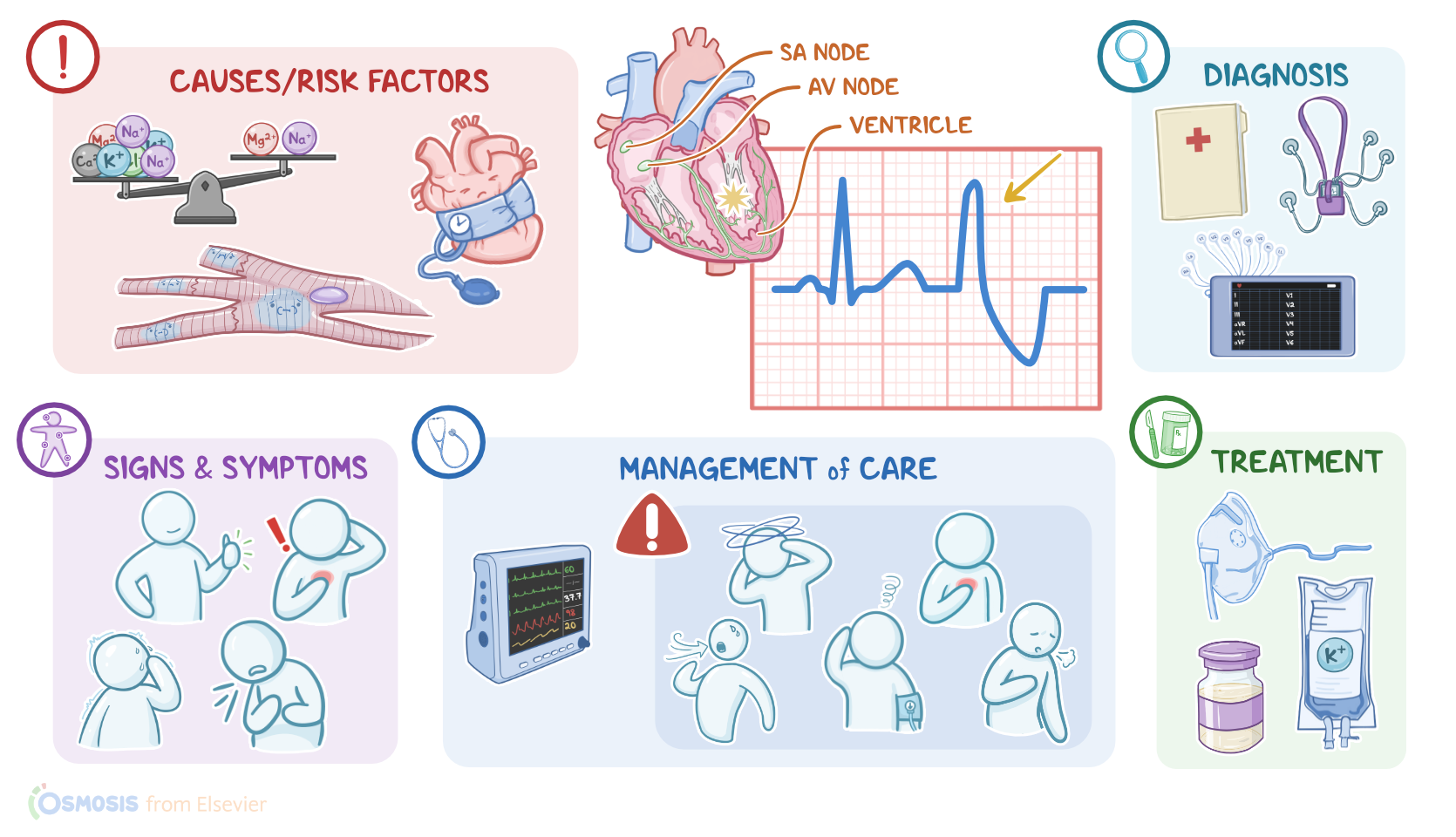
Premature ventricular contractions, or simply PVCs, are a type of arrhythmia, where an extra beat starts in a point in the ventricles, causing the ventricles to contract earlier than normal in the cardiac cycle. Now let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat. The normal electrical activity of the heart starts in the sinoatrial or SA node, which is considered the pacemaker of the heart. Then, the impulse is conducted through the atrium, creating the P wave on an ECG. And when the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles.
From the atrium, electrical activity goes to the atrioventricular, or AV node, where the impulse propagation speed slows way down; this is the PR interval on an ECG. This pause allows the atria to contract while the ventricles fill with blood. From the AV node, the depolarization wave goes through the Bundle of His, then the right and left branches of the Bundle, and finally through the Purkinje fibers, which deliver the current to the right and left ventricles, causing them to depolarize. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations, and it’s represented by the QRS complex on an ECG.
Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole. And on ECG, ventricular repolarization will create a T wave, while the pause between ventricular depolarization and repolarization is represented by the ST segment. Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles. Now, the 3 main causes of premature ventricular contractions are enhanced automaticity, triggered activity, and reentry. Now, automaticity is the property of cells in the SA node, AV node, Bundle of His, and the Purkinje fibers to generate an electrical impulse, so they’re all pacemakers but follow the SA node’s lead. However, when there’s a stressor that irritates the pacemaker cells in the ventricles, it could enhance their automaticity and cause them to fire early.
Risk factors can include electrolyte imbalance like hypokalemia and hypomagnesemia, damage to cardiac tissue like ischemia, and anything that increases sympathetic activity like hyperthyroidism, anxiety, or substances like caffeine or methamphetamine. Next, there’s triggered activity where a previous impulse causes an additional depolarization in the ventricle called an “after-depolarization” and this can occur in a pattern, like once after every other beat. The cause of it is not fully understood but it’s likely due to dysfunctional ion channels or injury to cardiac tissue. A final type of ventricular ectopic focus is a reentrant loop, where a depolarization wave encounters tissue that doesn’t depolarize, which can be something like scar tissue after a myocardial infarction, and as a result the wave starts going around and around that tissue - forming what’s called a reentrant loop.
Risk factors of premature ventricular contractions can be modifiable or non-modifiable. Modifiable risk factors include electrolyte imbalances, and underlying cardiovascular disease, including hypertension. On the other hand, non-modifiable risk factors include being assigned male at birth, black race, and advanced age. Now, regardless of the cause of the premature ventricular contraction it will lead to a pathological process that disrupts the normal heart rhythm. This depends on when the ectopic PVC occurs. So, the impulse from the ectopic beat typically travels back up to the atrium and this is called a retrograde conduction. If the ectopic beat happens right after the atrium has just depolarized, the cells in the conduction pathway are in its refractory period, so the impulse doesn’t make it pass the AV node, so there’s no extra atrial or ventricular contraction.
When the SA node fires again, the heart returns to sinus rhythm. On the other hand, if the ectopic beat occurs later, then the atrium could already be out of its refractory period, so the retrograde conduction will cause an extra atrial contraction. Furthermore, when the impulse reaches the SA node it’ll cause a depolarization after the atrium’s already contracted, so the impulse doesn’t go anywhere and it essentially resets the node. Clients with premature ventricular contractions are typically asymptomatic, but some clients present with palpitations, diminished or absent peripheral pulses, in addition to feeling that the heart skips a beat, which is typically followed by a fluttering sensation. Other signs and symptoms include anxiety, lightheadedness, dyspnea, and chest pain.
The diagnosis of premature ventricular contractions starts with the client's history and physical assessment, followed by cardiac monitoring using an electrocardiogram or a Holter monitor, which is basically a portable ECG that records for a 24-hour period. So, on the ECG, the heart rate may vary depending on the intrinsic rate and the number of PVCs, and the rhythm can be irregular. Keep in mind P waves are rarely seen right before a premature ventricular contraction and, as a consequence, PR intervals can’t be measured. Sometimes, P waves are seen after a PVC, which is caused by retrograde conduction of the ectopic impulse to the atria. The QRS complex is typically wide and distorted, meaning that it lasts for more than 0.12 seconds. On the other hand, T waves are typically larger and are opposite to the direction of the QRS complex.