Arrhythmias - Sinus tachycardia and sinus bradycardia: Nursing
Arrhythmias - Sinus tachycardia and sinus bradycardia: Nursing
Acute Final
Acute Final
Notes
| ARRHYTHMIAS - SINUS TACHYCARDIA AND SINUS BRADYCARDIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Arrhythmias are irregular heartbeats that occur due to any disturbance in the rate, rhythm, site of origin, or conduction of the cardiac electrical impulse, which can affect the heart’s ability to effectively pump blood throughout the body.
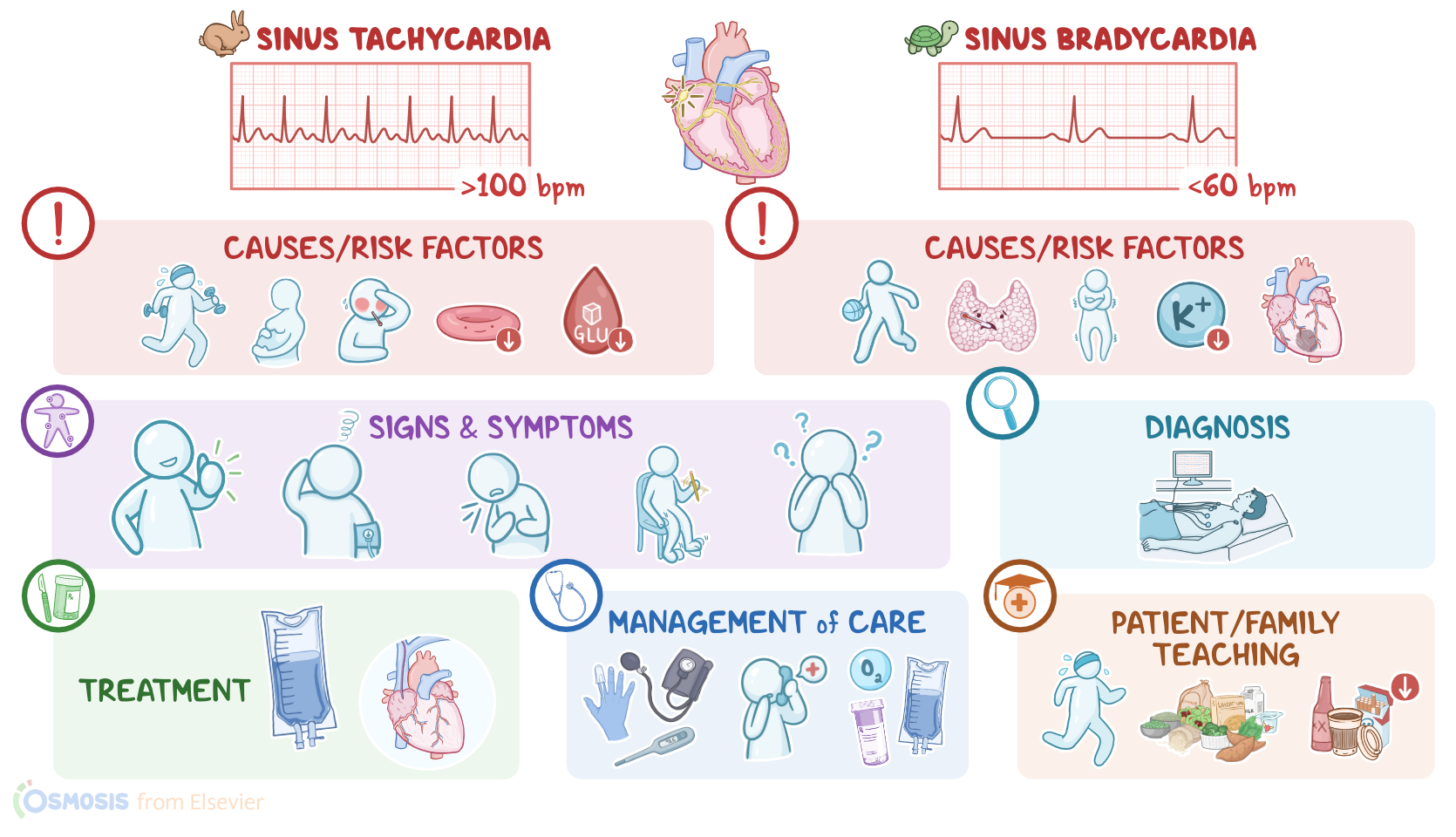
In sinus tachycardia and sinus bradycardia, the electrical impulse originates where it should, in the sinoatrial node, but the node fires either too fast or too slow. The cardiac rhythm is normal, meaning the beats are spaced evenly apart, but in sinus tachycardia the heart rate is more than 100 beats per minute, while in sinus bradycardia, it is less than 60 beats per minute.
Now, the cardiac conduction system is made up of specialized myocardial cells that can create and transport electrical potential, also called an action potential. These cells have many special features, including automaticity, meaning that they can generate an impulse; excitability, which is the ability to respond to a stimulus by creating an electrical impulse; conductivity meaning they can carry the impulse to other cells; and contractility, which is the ability to shorten the length of their fibers, causing a contraction.
Let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat.
The normal electrical activity of the heart starts in the sinoatrial node or SA node, which is considered the pacemaker of the heart.
Then, the impulse is conducted through the atria, causing depolarization and creating the P wave on an ECG. When the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles.
From the atria, the impulse goes to the atrioventricular node, or AV node, where the impulse propagation speed slows way down. The interval from the atrial depolarization to just before ventricular depolarization is the PR interval on an ECG. This delay allows the atria to contract while the ventricles fill with blood.
From the AV node, the impulse goes through the Bundle of His, then to the right and left bundle branches, and finally through the Purkinje fibers, which deliver the impulse to the right and left ventricles, causing them to depolarize, and is represented by the QRS complex on an ECG. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations.
Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole. And on ECG, ventricular repolarization will create a T wave, while the phase between ventricular depolarization and repolarization is represented by the ST segment. Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles.
Finally, to figure out the heart rate on an ECG, we can count the number of QRS complexes in six seconds and multiply that by 10. This normally lies between 60 and 100 beats per minute. The heart rate is mainly regulated by the autonomic nervous system. Specifically, the sympathetic nervous system increases the heart rate, while the parasympathetic nervous system decreases it. These two systems oppose each other’s actions so that a normal heart rate can be maintained under regular circumstances.
Now, let’s look at sinus tachycardia, which is typically caused by sympathetic nervous system stimulation, or parasympathetic nervous system inhibition. Sinus tachycardia can be normal during exercise and pregnancy and can also occur as a physiological response to fear or pain.
Pathological causes include fever, anemia, electrolyte abnormalities, as well as hypoglycemia, hyperthyroidism, hypotension, hypovolemia, and hypoxia.
In addition, caffeine, cocaine, and amphetamine, as well as various medications can also lead to sinus tachycardia. These include epinephrine, norepinephrine, atropine, theophylline, hydralazine, and some over the counter cold medications that contain pseudoephedrine.
Finally, withdrawal from alcohol or medications like benzodiazepines can also cause sinus tachycardia.
Okay, on the other side of the spectrum we have sinus bradycardia, which can be caused by parasympathetic nervous system stimulation, or sympathetic nervous system inhibition. Of note, sinus bradycardia, can be completely normal in athletes, and it’s also normal during sleep.
Pathological causes of sinus bradycardia include hypothyroidism, hypothermia, hypokalemia, and inferior wall myocardial infarctions, as well as increased intracranial pressure, which can be due to head trauma, strokes, and brain tumors. In addition, medications like beta blockers, calcium channel blockers, and opiates can cause sinus bradycardia.
Now, the pathology of sinus tachycardia starts with stimulation of the sympathetic system or inhibition of the parasympathetic system, which causes increased firing of impulses from the SA node. This increases the heart rate above 100 beats per minute, which initially increases cardiac output.
Over time, though, a fast heart rate decreases diastolic filling time, which, in turn, decreases the stroke volume or the volume of blood the left ventricle pumps with each heartbeat. At the same time, there’s an increased demand for oxygen by cardiac muscle cells. But since the perfusion of the myocardium by the coronary arteries occurs during diastole, sinus tachycardia also causes decreased myocardial perfusion.
On the other hand, the pathology of sinus bradycardia often starts with excessive parasympathetic stimulation, which causes decreased firing of impulses from the SA node. This leads to decreased heart rate, which increases diastolic filling time, which translates to increased coronary perfusion time. However, since the cardiac output is decreased, there’s also decreased coronary perfusion pressure, which once again decreases myocardial perfusion. In this case, though, there’s also a decreased demand for oxygen by cardiac muscle cells.
Complications linked to both sinus tachycardia and bradycardia include myocardial ischemia or infarction, heart failure, and cardiomyopathy.
Now, in terms of clinical manifestations, these can depend on the degree of tachycardia or bradycardia, and how well the client tolerates the altered heart rate, so some clients with these arrhythmias are asymptomatic. On the other hand, some can develop hypotension, dizziness, dyspnea, restlessness, confusion, palpitations, and even angina, or chest pain.
Sources
- "Critical care nursing: Diagnosis and management (10th ed.). ISBN: 978-0-443-11581-3 " Elsevier (2026)
- "Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. 12th Edition. ISBN:978-0-323-78961-5 " Elsevier
- "Guyton and Hall Textbook of Medical Physiology. ISBN 978-0323597128 " Elsevier (2020)
- "Mosby’s® Diagnostic and Laboratory Test Reference. 15th edition. ISBN: 978-0-323-67519-2 " Mosby (2020)
- "Saunders Comprehensive Review for the NCLEX-RN. 9th Edition. ISBN: 978-0-323-79530-2 " Saunders (2022)
- "Fundamentals of Nursing. 11th edition. ISBN: 978-0-323-81034-0 " Elsevier (2022)
- "Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. 11th Edition. ISBN: 978-0-323-55149-6 " Mosby (2019)
- "Continuous heart rate dynamics preceding in-hospital pulseless electrical activity or asystolic cardiac arrest of respiratory etiology. 179:1-8. " Resuscitation (2022)