Breast cancer: Nursing process (ADPIE)
Notes
| BREAST CANCER | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
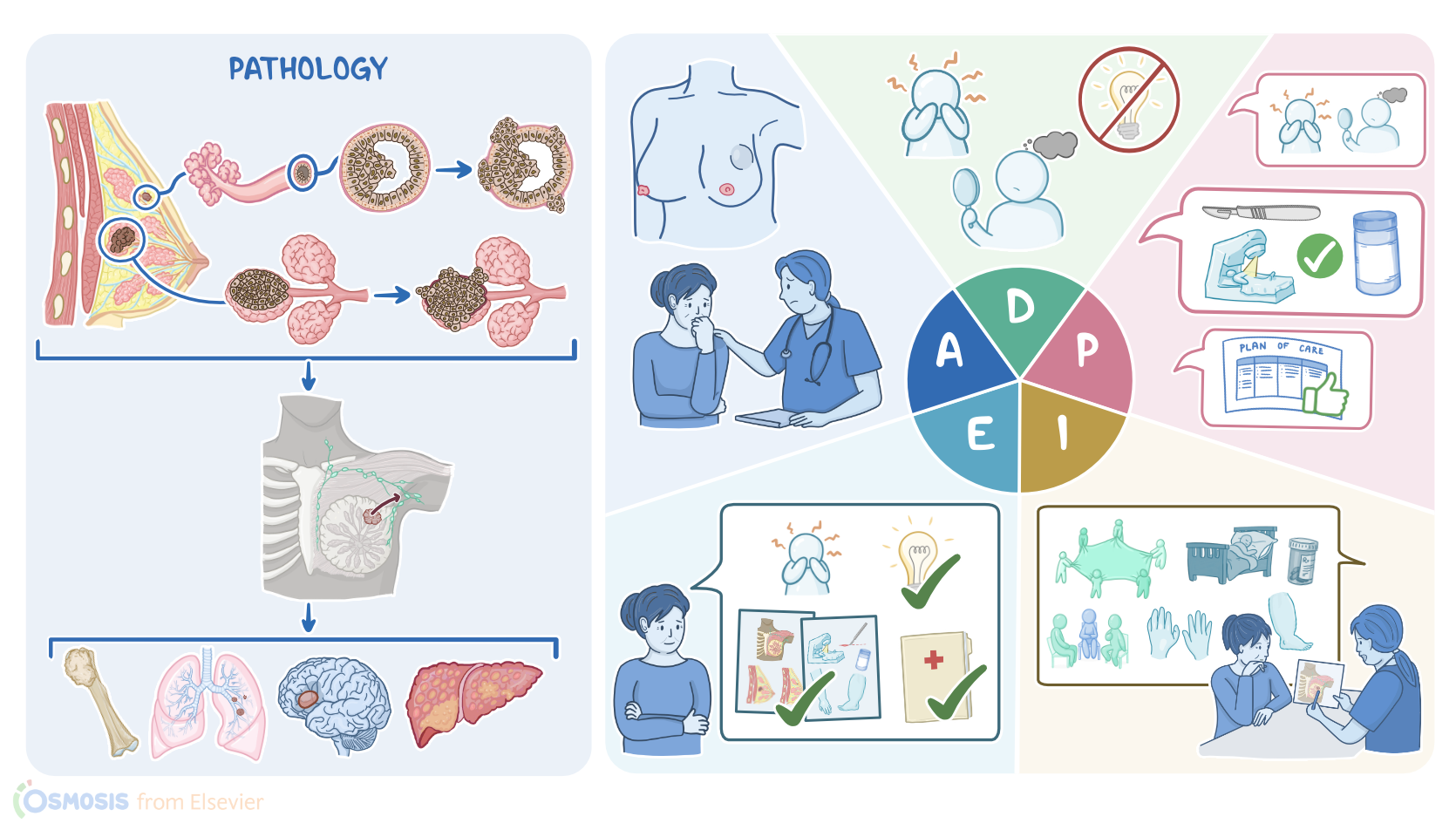
Linda Davis is a 54-year-old female client recently diagnosed with ductal carcinoma in situ, or DCIS. Because Ms. Davis’s mother had breast cancer, she was concerned when she felt a painless lump in her left breast during her monthly self breast exam.
A mammogram shows linear and branching areas of microcalcifications, so a percutaneous core needle biopsy is performed. Pathology reveals pleomorphic, high-grade nuclei, areas of central necrosis in the ducts without invasion of the basement membrane, and ER+/PR+/HER2- cells.
Ms. Davis presents to the oncology office for consultation. Breast cancer is the uncontrolled growth of epithelial cells within the breast tissue. It is the second most common cancer worldwide, and is also the second leading cause of cancer deaths in females, but on rare occasion, it may affect males.
Now, the female breasts are typically made up of glandular tissue, which consists of lobes containing numerous milk-producing lobules with a network of lactiferous ducts that transport milk to the nipple during lactation.
On the other hand, male breasts have ducts and some may have a few lobules that don’t produce milk. Now, this glandular tissue is surrounded by stroma, which is made of adipose and fibrous connective tissue.
Located throughout the breasts are blood vessels, as well as lymphatic vessels that mainly drain into a group of lymph nodes in the axilla.
Alright, now, most breast cancers are adenocarcinomas originating from the ducts or lobules, and can be categorized by whether or not they have invaded surrounding tissue.
Non-invasive, also called in situ, breast cancers are confined to the ducts, called ductal carcinoma in situ, or DCIS for short, or lobules, called lobular carcinoma in situ, or LCIS for short.
Some non-invasive breast cancers can become invasive breast cancers, which infiltrate the basement membrane and spread to surrounding tissue where they can reach the blood and lymphatic vessels, ultimately leading to metastasis.
The most common invasive breast cancers include invasive ductal carcinoma, which starts from the ducts, and invasive lobular carcinoma, which starts from the lobules.
Now, the exact cause of breast cancer is not fully understood, but is thought to be influenced by a variety of risk factors. The most common risk factors include age over 50, and family history of breast or ovarian cancer.
Other risk factors include hereditary genetic mutations in tumor suppressor genes, such as BRCA1, BRCA2, and less frequently TP53 or CHEK2, which normally control cell proliferation.
There’s also increased risk of breast cancer with increased estrogen exposure like nulliparity, first pregnancy after the age of 30, early menarche before the age of 12, and late menopause after the age of 55.
Other risk factors include absence of breastfeeding, obesity, as well as smoking, heavy alcohol consumption, and exposure to radiation. Finally, Caucasian individuals seem to be at the highest risk of breast cancer.
Generally, the first symptom of breast cancer is a hard, irregular, fixed or non-mobile, painless lump or swelling, most often located in the upper outer quadrant of the breast.
Skin may appear reddened, swollen, and be warm to touch, or present with ulceration. If the cancer cells obstruct the lymphatics, they can cause swelling and thickened skin around exaggerated hair follicles, giving the skin the appearance of an orange peel, also referred to as peau d'orange.
Paget disease occurs when cancer cells migrate along the lactiferous duct and through the pore, onto the skin over the nipple, and can cause itching, redness, crusting, and clear or bloody discharge from the nipple.
If not promptly treated, breast cancer can lead to complications like metastasis. Metastases often occur through the axillary lymph nodes, so clients may present with swelling and palpable nodes under the armpit.
Other common sites for metastasis include bones, lungs, brain, and liver. Unfortunately, most cases of metastatic breast cancer can’t be cured, so they eventually lead to death.
Diagnosis of breast cancer often begins with history and physical examination, followed by mammography. In addition, other imaging techniques like ultrasound and MRI may be done to detect the tumor and determine the TNM stage, which stands for tumor size, nodal involvement, and metastasis.
Finally, a biopsy of suspicious tissues or lymph nodes must be done to confirm the diagnosis and testing for the expression of hormone receptors, such as estrogen and progesterone receptors, or ER and PR for short, as well as human epidermal growth factor 2 or HER2 receptors.
In terms of screening, according to the American Cancer Society guidelines, females aged 45 to 54 years of age should undergo screening mammography every year.
Treatment for breast cancer is based on the type and TNM stage. Surgery is the mainstay of treatment whenever possible. Depending on their size, non-invasive tumors are removed surgically by either lumpectomy, or partial or total mastectomy.
In addition, nearby structures like lymph nodes may also be removed if the cancer has metastasized to them. Surgery can be followed by other local treatments like radiotherapy, as well as systemic therapy with chemotherapy or immunotherapy.
Other systemic therapies include hormonal therapy with tamoxifen, exemestane, or an aromatase inhibitor, for clients that are positive for ER or PR; as well as targeted therapy with trastuzumab for HER2 positive clients.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Customizing local and systemic therapies for women with early breast cancer: the St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021" Ann Oncol (2021)
- "Overcoming Endocrine Resistance in Breast Cancer" Cancer Cell (2020)
- "Global Increase in Breast Cancer Incidence: Risk Factors and Preventive Measures" Biomed Res Int (2022)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Molecular Classification of Breast Cancer" Adv Anat Pathol (2020)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)