Cervical cancer: Nursing
Cervical cancer: Nursing
Cellular and hormonal regulation
Cellular and hormonal regulation
Notes
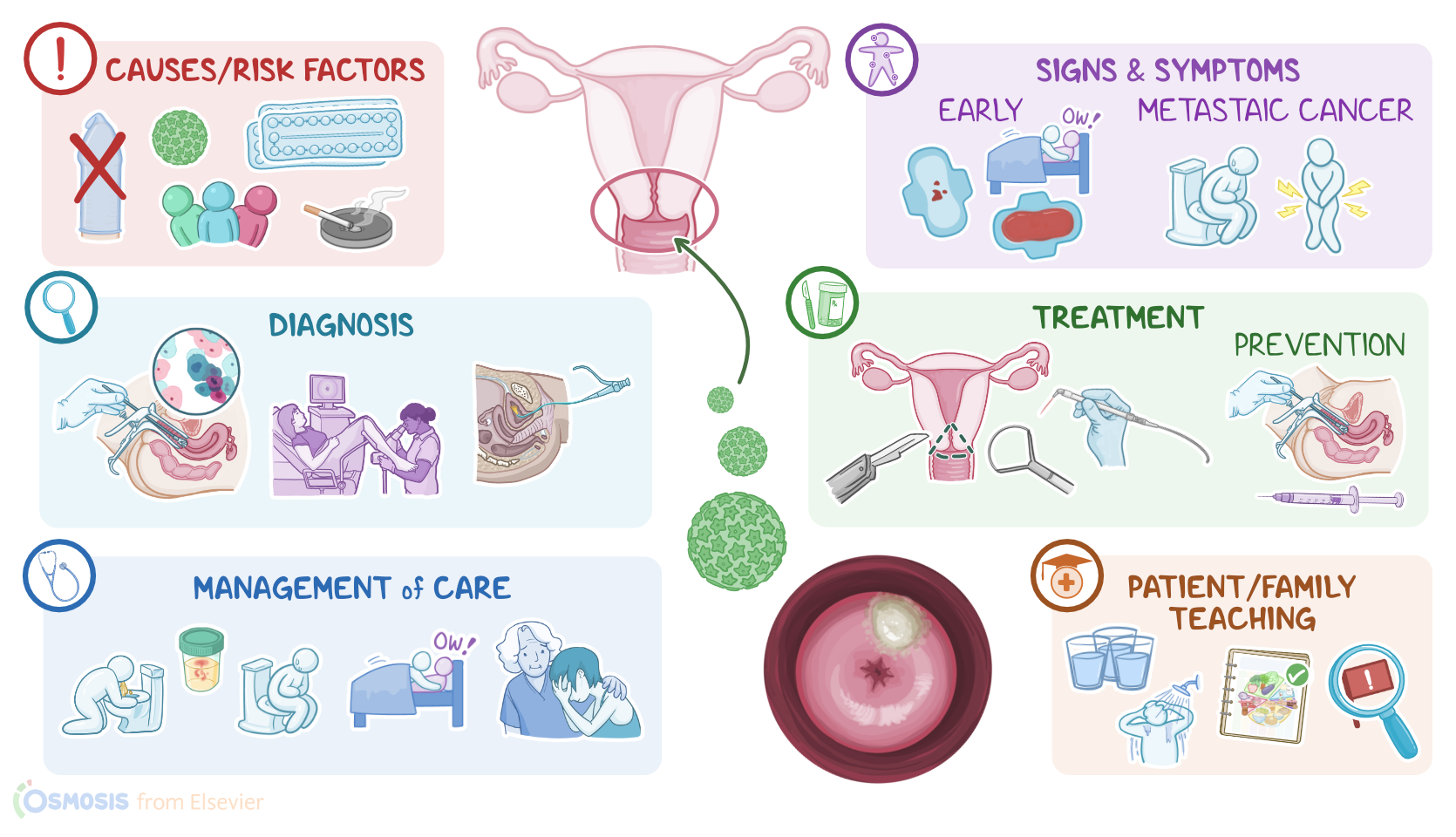
| CERVICAL CANCER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Cervical cancer is a malignant tumor that originates in the cervix, and is one of the most common types of cancer.
All right, now let’s go over some anatomy and physiology. The cervix is the lower part of the uterus, and can be divided into two sections; the inner part is called the endocervix, which is a narrow canal that leads into the uterus; while the outer part is called the ectocervix, and it sticks out into the vagina.
Zooming in, the endocervix is lined by mucus-secreting simple columnar epithelial cells. Conversely, the ectocervix is continuous with the vagina and is lined by stratified squamous epithelial cells. The area where the two epithelia meet is called the transformation zone, and it is where there is a change from columnar cells to squamous cells, called the squamocolumnar junction. The exact location of the squamocolumnar junction will change or shift depending on the age of the individual, as well as changes in the size of the uterus during menstruation.
Now, cervical cancer can arise due to a variety of causes and risk factors. Most cervical cancers are caused by human papillomavirus, or HPV for short. Specifically, high-risk HPV strains such as 16 and 18 are responsible for more than half of all cervical cancers. Since HPV is a sexually transmitted infection, the risk of developing cervical cancer is higher in clients who engage in unprotected sex or who have multiple sexual partners. Additional risk factors include early age at first sexual intercourse, smoking, having a compromised immune system, obesity, long-term use of oral contraceptive pills, as well as having a family history of cervical cancer.
Now, it’s important to note that not all HPV infections result in cervical cancer. In fact, the immune system is able to fight off most HPV infections so they don’t cause any serious harm. When that doesn’t happen, though, the virus inserts itself into the immature squamous cells of the transformation zone, leading to changes in the cell’s DNA. As a result, infected cervical epithelial cells undergo dysplasia, or abnormal growth, which can lead to the formation of a precancerous lesion called cervical intraepithelial neoplasia.
Depending on how much of the epithelium is affected by dysplasia, cervical intraepithelial neoplasia can be divided into three grades. The higher the grade, the more likely the lesion will evolve into cancer. Eventually, cervical intraepithelial neoplasia can evolve into carcinoma in situ, which affects the entire thickness of the epithelium. Finally, carcinoma in situ can progress to invasive squamous cell carcinoma, which is when cancerous cells break through the epithelial basement membrane, into the cervical stroma, and may even spread or metastasize to neighboring tissues and organs, such as the vagina, uterus, or pelvic wall, as well as to other areas of the body.
Less frequently, HPV infects the mucus-secreting columnar cells, giving rise to adenocarcinoma in situ, which may progress to invasive cervical adenocarcinoma.
Early cervical cancer doesn’t typically cause any symptoms. The first symptom is often painless vaginal bleeding, especially after sexual intercourse, as well as menorrhagia or abnormally heavy or prolonged menstrual periods. Other symptoms include spotting between periods, foul-smelling vaginal discharge, vaginal discomfort, and dyspareunia or painful intercourse. Finally, in case of metastatic cancer that has spread beyond the cervix, the client may experience symptoms like pelvic pain, constipation, and frequent, painful, or bloody urination, as well as general symptoms like weight loss.
Diagnosis of an asymptomatic client involves screening with HPV DNA testing, along with a Pap smear, or Papanicolau test, where a sample of cells from the transformation zone is collected with a brush and then examined under a microscope. If the Pap smear shows evidence of abnormal cell changes like dysplasia, it will be followed up with a colposcopy, which is when a magnifying device called a colposcope is used to examine the cervix, and then obtain biopsies to confirm the diagnosis.
Afterwards, imaging tests like a CT scan or MRI, as well as endoscopic tests like cystoscopy or rectosigmoidoscopy, can be done to look for evidence of metastasis. Once diagnosis is confirmed, cervical cancer can be staged using the FIGO system, which is based on findings from pelvic examination, cervical biopsy, imaging, and endoscopic studies.
Treatment options for cervical cancer depend on the aggressiveness and extension of the tumor. Precancerous lesions can be destroyed with local ablation modalities, such as cryosurgery or laser surgery. Small, localized tumors can be treated with conization, which is when the transformation zone and part of the endocervix are removed surgically. This can either be done with a scalpel, called cold-knife conization, or by heating a loop of thin wire with electricity, called loop electrosurgical excision procedure, or LEEP. On the other hand, treatment of larger tumors typically involves hysterectomy, or surgical removal of the uterus, and removal of associated lymph nodes.
For metastatic cancer, treatment generally involves more extensive surgeries, along with chemotherapy and radiotherapy. Finally, the most effective way to prevent cervical cancer is through HPV vaccination and regular screening.
All right, let’s look at the nursing care you’ll be providing for a client with cervical cancer. Nursing goals focus on administering chemotherapeutic medications and managing side effects, as well as providing post-operative care, and providing comfort and emotional support to promote quality of life.
First, perform a pain assessment, including the onset, quality, severity, location, aggravating or relieving factors, and how frequently they experience pain. Be sure to assist your client into a comfortable position, provide comfort measures, and administer analgesics as prescribed. If your client’s pain is unrelieved with medication, report these findings to the healthcare provider.