Chickenpox (Varicella): Nursing process (ADPIE)
Client Report0:00–0:25
15 month old Lilian Becker presents with a vesicular rash to her trunk and arms. Itchiness and fever.
Onset of symptoms occurred after being picked up from daycare two days ago. After being brought into the pediatric clinic by her father, Ray, Lillian is diagnosed with chickenpox.
Pathology0:25–6:35
Varicella, more commonly referred to as chickenpox, is an infectious disease caused by the varicella zoster virus, or VZV for short, also known as human herpes virus 3 or HHV3 for short.
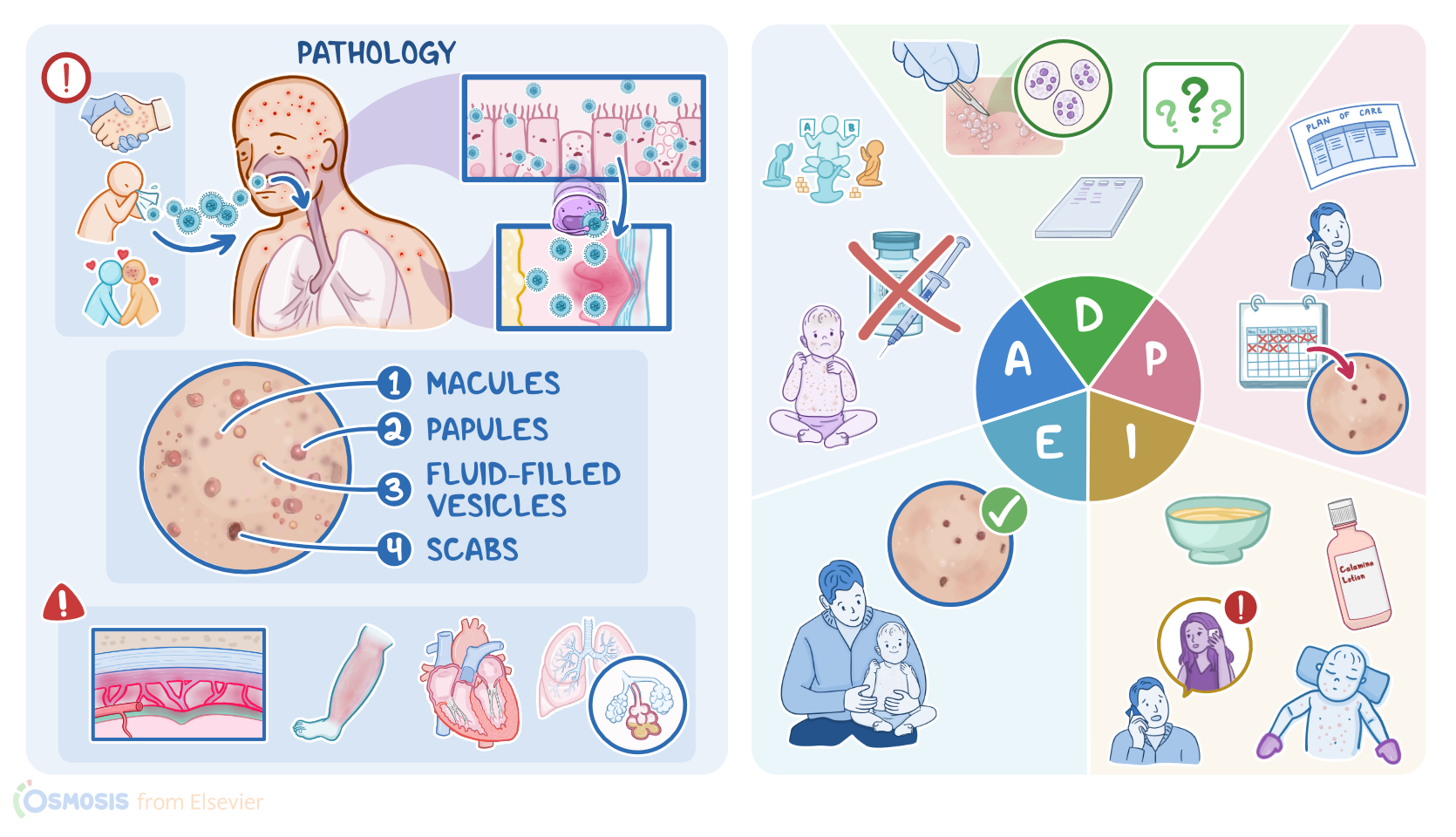
This is a highly contagious airborne virus, meaning it's transmitted from person to person through respiratory droplets.
For example, when a person sneezes or coughs. But the virus can also be transmitted by direct contact with the skin or oral mucosa of an infected person.
Now, once a person inhales the virus-containing droplets, these travel down the respiratory mucosa and the virus starts replicating in the epithelial cells.
This is called the incubation period, where the client is asymptomatic and lasts 14 to 21 days. Then the virus gets picked up by nearby immune cells and gets transported to a nearby lymph node, so the client may start to experience prodromal symptoms such as fever, headache, and malaise.
Prodromal symptoms are more likely in clients over the age of 10 and more severe in adults. About 36 to 48 hours later, the immune cells reach the skin and release the virus.
At this point, clients typically develop skin lesions, usually involving the scalp, face, and trunk. Initially, skin lesions appear as flat, red, and very itchy spots called macules.
Over time, macules become elevated and progress into papules, and then into small fluid-filled vesicles. Within 1 to 2 days, these vesicles begin to crust over and form scabs.
After 5 days, the scabs fall off, typically without leaving a scar, unless the client picks or scratches their skin. Now, every 3 to 5 days, new crops of lesions form in different places on the body, so it's possible to see skin changes in different phases at the same time.
Now, most clients have chickenpox only once and will develop immunity against it for the rest of their lives. However, varicella zoster virus also infects sensory neurons in the skin and travels backward, or retrogradely through the neuron to the dorsal root ganglia and trigeminal ganglion.
Over time, when the immune system kicks in, most of the viruses in the body are eliminated, but the ones in the ganglion are spared and can remain dormant in the latent state for many years.
Later on, if the immune system weakens due to aging, stress, or immunosuppressive therapy, the virus can be reactivated and travel back up or anterogradely through the sensory nerve to the skin.
Causing an infection in the innervated dermatome that's called herpes zoster or shingles. Now, both chickenpox and shingles can cause some serious complications.
The most common one is a secondary bacterial infection of the skin lesions causing cellulitis. Other complications include hepatitis, myocarditis, and pneumonia, as well as hemorrhagic complications such as febrile purpura.
Purpura refers to the discoloration of the skin and mucous membranes due to small blood vessel hemorrhage. Finally, chickenpox can affect the central nervous system.
First, it can cause acute post-infectious cerebellar ataxia, which refers to a sudden onset of ataxia following a viral infection.
It can also cause meningitis or inflammation of the meninges and transverse myelitis or inflammation of the spinal cord.
Finally, children treated with aspirin may develop Ray syndrome, which is characterized by hepatic encephalopathy. Now, diagnosis of chickenpox is usually based on clinical findings and can be confirmed using PCR to detect viral DNA.
In addition, a zonk test or smear can be performed by scraping a skin lesion to look for multinucleated giant cells in the fluid of the vesicles.
Finally, chickenpox can be diagnosed if a client has IgM antibodies against the varicella zoster virus or if Varicella zoster antigens are detected by immunofluorescence.
Treatment of chickenpox includes cool baths or calamine lotions to help reduce the itching. Also, analgesics and anti-inflammatory medications can help reduce the fever, but aspirin shouldn't be used in someone with chickenpox because it can trigger Ray syndrome.
In addition, clients aged 12 or over can be treated with oral antiviral medications like valacyclovir or famcyclovir. On the flip side, immunocompromised clients and those at risk of developing severe disease require intravenous administration of acyclovir.
The good news is that chickenpox can be prevented with vaccination. Now, let's begin our assessment to learn more about Lillian's current condition.
Assessment6:35–8:05
After donning the appropriate personal protective equipment, you ask Ray to share about Lilian's symptoms. Ray tells you that what started off as mild red bumps scattered across her abdomen, gradually turned into inflamed, blister-like bumps that started spreading.
Assessment of Lillian's trunk and arms reveals vesicular lesions, some of which appear to be very erythemic and actively oozing clear fluid.
You also note macules are present on Lilian's upper neck and cheeks. Her oral mucosa appears intact without any notable sores.
During your assessment, Lilian attempts to scratch at the lesions, and Ray confirms that she scratches at the affected sites, even when she's asleep.
Lillian has not yet received the varicella vaccination, and Ray expresses worry about the other families at the daycare center who also have not had their children vaccinated.
Lilian's vital signs are tympanic temperature 100.4 °F or 38 °C, heart rate 90 BPM, respirations, 24 breaths per minute, BP, 95/60 millimeters of mercury, and oxygen saturation, 97% on room air.
With the data you've collected, you are now able to create the following priority nursing diagnoses impaired skin integrity related to presence of lesions, risk of secondary bacterial infection related to puritis, and readiness for enhanced parental learning related to a new diagnosis.
Diagnosis8:05–8:25
After collaborating with Lilian's pediatrician and Ray, you establish a plan of care for Lilian. In 10 days, Lilian's lesions will be crusted over and healing well.
Planning8:25–8:48
There will be no signs of symptoms of secondary bacterial infection, and Ray will demonstrate how to care for Lilian at home and prevent spread of infection to the community.
It is now time to begin implementing Lilian's plan of care. To promote adequate healing of the lesions, you teach Ray the importance of Lilian having adequate rest, nutrition, and hydration.
Implementation8:48–10:32
You also encourage frequent washing of Lilian's hands, clothing, and bedding to help prevent the spread of lesions. You explain that cool baths without soap or bubble bath, calamine lotion, and use of child-approved oral antihistamines like diphenhydramine or Benadryl can help alleviate Lillian's pruritis.
You show Ray how to keep Lilian's nails carefully trimmed and recommend having her wear mittens while asleep to help prevent further skin irritation from scratching.
Next, you ensure that Ray knows how to safely manage Lillian's fever with the use of antipyretic medications such as acetaminophen or ibuprofen, and avoid use of aspirin.
After this, you provide Ray with resources on pediatric immunizations and the recommended timetables. You and Ray discussed the importance of notifying the daycare center of Lilian's infection and isolating at home until all Lilian's lesions are crusted over.
After answering his questions, you encourage Ray to contact the pediatrician if he notices the affected sites become very warm, erythemic, or edematous.
If lesions form near Lilian's eyes, or if she develops a fever of 102 °F or 38.9 °C. It's been 10 days since Lillian was first diagnosed with chickenpox, so let's check in with her and Ray to evaluate how things have been going.
Evaluation10:32–11:53
Direct observation shows crusty lesions that appear to be healing well. No new macules or oozing vesicular lesions are present body-wide.
You do not note any signs or symptoms of secondary bacterial infection. Lillian has not attempted to scratch the affected sites lately, and Ray tells you that the calamine lotion is working well to manage her puritis.
Lillian's vital signs are tympanic temperature 98.4 °F or 36.8 °C, heart rate, 88 BPM, respirations, 26 breaths per minute, BP, 92/54 millimeters of mercury, and oxygen saturation, 99% on room air.
Ray shares that he has been communicating with the other affected daycare families on the importance of isolating to prevent further outbreaks from occurring throughout the surrounding community.
You're glad that Lilian is recovering well and that Ray is sharing his knowledge within the daycare community. All right, as a quick recap, Lillian Becker presented to the pediatric clinic with signs and symptoms of chickenpox, which is an infectious disease caused by the varicella zoster virus.
Summary11:53–12:44
Your assessment revealed vesicular lesions, puritis, and fever. The priority nursing diagnoses you established were impaired skin integrity, risk of secondary bacterial infection.
And readiness for enhanced parental learning. Careful planning allowed you to create goals that focused on alleviating Lillian's symptoms and teaching Ray how to prevent spread of the disease.
Implementation of the plan of care involved improving Lillian's skin integrity and providing Ray with resources. Finally, you evaluated that Lillian's plan of care was effective in promoting her well-being.
| CHICKENPOX (VARICELLA) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
- "Definition, Causes, Pathogenesis, and Consequences of Chronic Obstructive Pulmonary Disease Exacerbations" Clin Chest Med (2020)
- "Assessing the use of antibiotics in pediatric patients hospitalized for varicella" Ital J Pediatr (2022)
- "Chickenpox in skin of color" Visual Journal of Emergency Medicine (2023)
- "How to differentiate skin rash in covid, mononucleosis, chickenpox, sixth disease and measles" Curr Opin Infect Dis (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Prevention of Herpes Zoster: A Focus on the Effectiveness and Safety of Herpes Zoster Vaccines" Viruses (2022)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
No notes for this video yet
Try adding a note below