Complete metabolic panel (CMP) - Blood urea nitrogen (BUN) and creatinine (Cr): Nursing
1,149views
Complete metabolic panel (CMP) - Blood urea nitrogen (BUN) and creatinine (Cr): Nursing
Renal/Urinary
Renal/Urinary
Notes
| BLOOD UREA NITROGEN (BUN) AND CREATININE (Cr) | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| PATHOLOGY |
| |
| NURSING IMPLICATIONS |
| |
Transcript
An elderly client is brought to the emergency department by ambulance, accompanied by his daughter, who reports her father has a history of systolic heart failure, that he’s been experiencing nausea, vomiting, and confusion. On assessment, there’s jugular vein distension, crackles on lung auscultation, and leg edema. Based on these findings, blood urea nitrogen or BUN, and creatinine are ordered to check the client’s renal function.
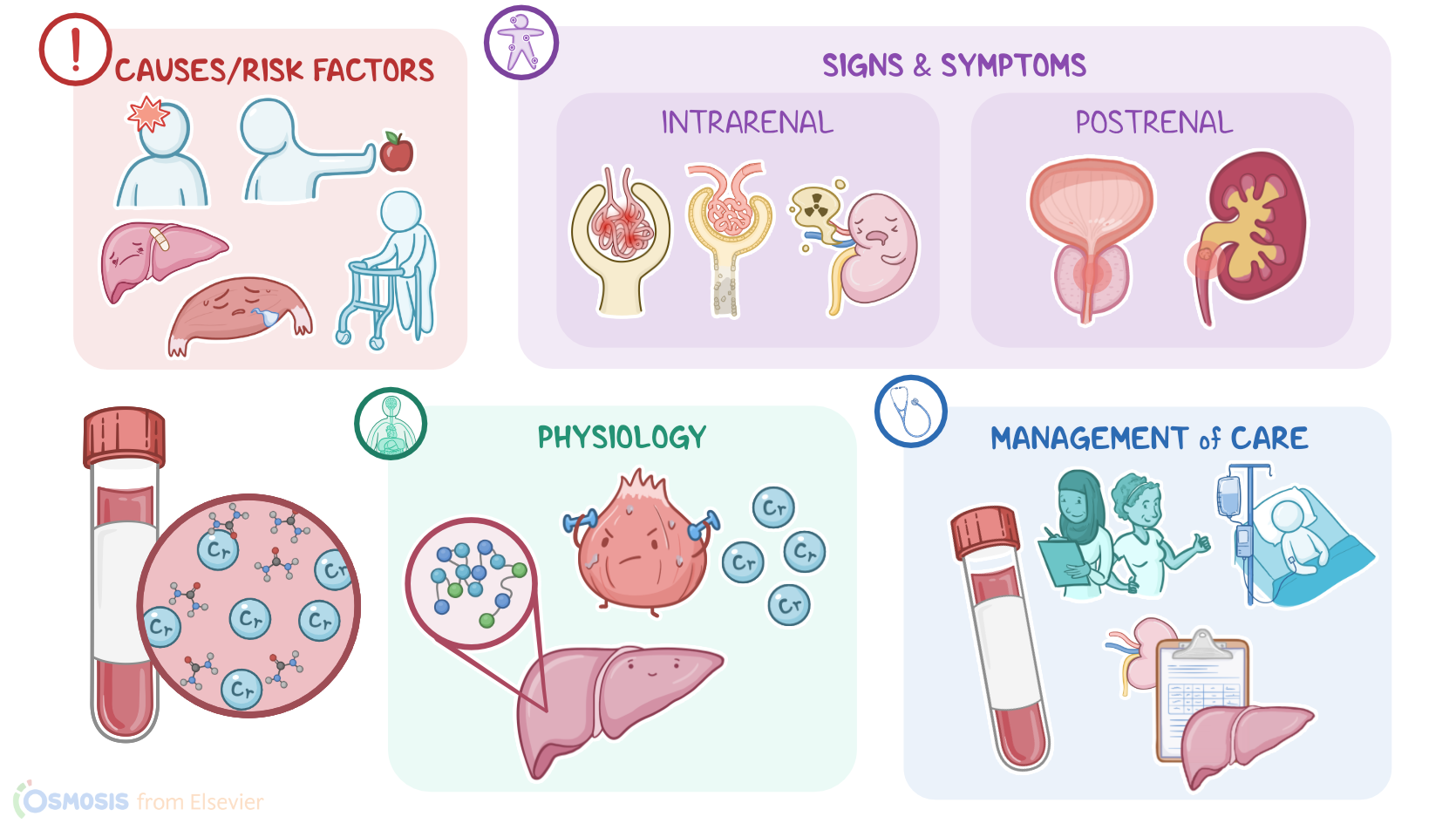
Alright, blood urea nitrogen, also known as urea nitrogen or just BUN, measures the blood level of urea nitrogen, which is a substance formed in the liver from protein metabolism. Most urea nitrogen is excreted in urine after filtration in kidneys, and only a small amount is reabsorbed.
Serum creatinine, abbreviated Cr, is a by-product of muscle contraction, and it’s made at a relatively constant rate as part of regular, everyday activity. All of the creatinine produced by the body is eliminated by the kidneys, with no reabsorption.
Because both urea and creatinine are eliminated by the kidneys, they are used to evaluate renal function. Also, to more closely determine the cause, the BUN to creatinine ratio is examined.
Now, BUN and creatinine can be drawn on their own, or as a part of the basic metabolic panel, or BMP, also known as the complete metabolic panel, or CMP. The normal value for BUN is 5 to 20 mg/dL. On the other hand, creatinine values tend to be higher in males, who tend to have a larger muscle mass. So, in healthy males, creatinine ranges from 0.7 to 1.3 mg/dL, while in females, it ranges from 0.6 to 1.1 mg/dL. Lastly, the BUN to creatinine ratio is somewhere between 10:1 and 20:1.
Alright, let’s switch gears and talk about conditions that can alter the client's BUN, which can be non-renal or renal. So, for non-renal conditions, the amount of urea nitrogen in the blood level is related to how much urea is produced by the liver. It will rise when the liver metabolizes more protein, like with increased protein intake or when there’s tissue breakdown, like with trauma or gastrointestinal bleeding. Conversely, the BUN will decrease in conditions like malnutrition, because there’s less protein for the liver to process. It will also decrease if the liver is impaired, since the liver isn’t able to metabolize the available protein, and in conditions of fluid overload, since the plasma becomes diluted.
As for renal issues, the BUN can change due to prerenal, intrarenal, and postrenal conditions. First, for prerenal conditions, anything that causes decreased blood flow to the kidneys can cause the BUN to rise. That’s because the BUN has an inverse relationship with the glomerular filtration rate, or GFR, which is how much blood the kidneys filter in one minute. So, as the GFR decreases, the BUN increases, since less renal blood flow means less filtration, less excretion of urea nitrogen, and more of it staying in the blood. Conditions that decrease the GFR include shock, heart failure, hypovolemia, and dehydration.
Next, intrarenal issues like glomerulonephritis, acute tubular necrosis, or the effects of nephrotoxic drugs will cause the BUN to rise.
Finally, postrenal conditions that stop the flow of urine, such as benign prostatic hyperplasia and kidney stones will result in an increased BUN.
Okay, let’s move on to conditions that can alter a client’s creatinine, which can be non-renal and renal. Now, because creatinine is made by the muscles at a relatively constant rate, a non-renal cause of a creatinine increase is when there's an extremely large muscle mass, like with bodybuilders. Conversely, a decrease in creatinine can result from decreased muscle mass, which can happen in conditions like muscular dystrophy or with elderly or debilitated clients. And like BUN, creatinine also has an inverse relationship with the GFR, so it will increase with any condition that causes the GFR to fall. However, the most important factors that increase creatinine are intrarenal, or any condition that damages the kidneys. This makes creatinine a much more sensitive indicator of renal function than BUN.