Complete metabolic panel (CMP) - Sodium: Nursing
Notes
| SODIUM | ||
| KEY POINTS | NOTES | |
| PHYSIOLOGY |
| |
| HYPERNATREMIA |
| |
| HYPONATREMIA |
| |
| INDICATIONS |
| |
| NURSING IMPLICATIONS |
| |
Transcript
Ms. Blanco is an older adult client who has been lethargic for the past few hours and arrives at the emergency department via ambulance. During the previous three days, she had recurrent episodes of diarrhea due to gastroenteritis. Her family reports that during this time they encouraged Ms. Blanco to drink lots of water to keep hydrated. On physical assessment, Ms. Blanco has dry mucous membranes, sunken eyes, tachypnea, and tachycardia. Based on these findings, a complete metabolic panel, or CMP, is ordered to check her electrolyte levels, including sodium. Now, sodium is a positively charged ion, or cation, which is abbreviated as Na+. It is the major cation in the body, and most of it is located outside the cells in the extracellular fluid. It is the major factor in the fluid's osmolality, which is the concentration of dissolved particles, including sodium and other electrolytes. Sodium is also a major determinant of how fluid is distributed around the body, and it helps maintain enough circulating volume for adequate tissue perfusion.
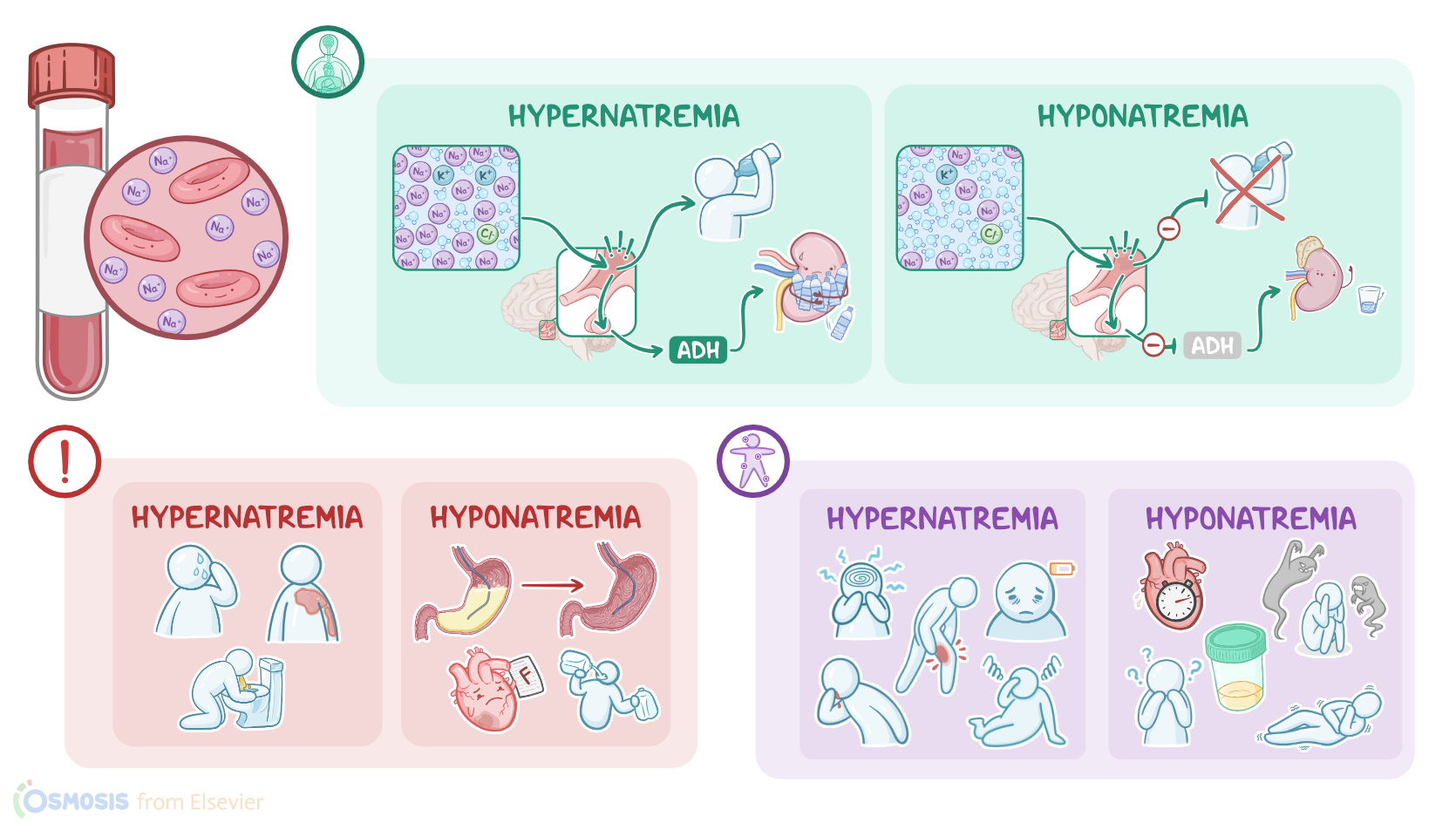
In addition, sodium is essential for the conduction of nerve impulses and muscle contraction. Together with chloride and bicarbonate, sodium helps to maintain acid-base balance. Sodium is introduced into the body through a person’s diet, especially when foods high in sodium are consumed, such as canned soup, tomato juice, processed meats, canned tuna, salted crackers, and cheese. Once ingested, sodium is absorbed in the blood by the gastrointestinal tract, and travels through the bloodstream. Then, most of the sodium is excreted through the kidneys, but a lesser amount is excreted through sweat and feces. Now, maintaining a normal sodium concentration is essential to keep our bodies functioning normally. When there’s hypernatremia, or a high sodium level, the serum osmolality also increases. The increased osmolality is detected by the osmoreceptors in the thirst center of the hypothalamus. In response, it stimulates the pituitary to release ADH, or antidiuretic hormone, into the blood. ADH then travels to the kidneys to increase water reabsorption back into the blood, so less water is lost in the urine.
The osmoreceptors also trigger the sensation of thirst, which causes the person to want to drink water. Together, the release of ADH and increased fluid intake help restore serum osmolality. On the other hand, when there’s hyponatremia, or a low sodium level, the sensation of thirst decreases, ADH is suppressed, and renal water excretion increases. Now, the plasma level of sodium can be measured on its own or as part of a complete metabolic panel or CMP, or a basic metabolic panel, also called a BMP. The sodium level result doesn’t necessarily reflect the total amount of sodium in the body but rather the amount of sodium relative to the amount of water in the body, known as the concentration of sodium. In adults, normal sodium levels range from 136 to 145 mEq/L. All right, now there are certain conditions that can cause hypernatremia. The most common clinical situation is excessive water loss. This can happen when water is lost through the skin, either from excessive sweating or due to extensive burns; through gastrointestinal losses, like with prolonged vomiting or diarrhea; or through the kidneys because of an increase in diuresis, like with diabetes insipidus, which happens when the body doesn't produce ADH.
Hypernatremia can also occur due to decreased intake of water, like in situations where access to water or the ability to drink water is limited, which can happen with elderly clients in nursing homes, for example. Finally, excessive sodium gain is a rare cause of hypernatremia, and it usually happens because of an iatrogenic sodium overload, like when hypertonic saline is administered. Now, clinical manifestations of hypernatremia are caused when the high level of sodium in the extracellular space causes fluid to shift from the inside of the cells to outside the cells - remember, water follows salt! As fluid leaves the cells, you may also notice neurological symptoms as fluid shifts out of brain cells, including lethargy, altered mental status, and irritability, and even seizures and coma. Neuromuscular irritability can also occur, so twitching or cramping can be present. Lastly, when hyponatremia is caused by water loss, you may notice signs of dehydration, like orthostatic hypotension, decreased skin turgor, and dry mucous membranes, as well as flushed skin and extreme thirst. .
Okay, now one type of hyponatremia is hypovolemic hyponatremia, which can occur when sodium loss is greater than water loss. This can occur with problems like diarrhea, vomiting, or gastrointestinal suctioning without fluid replacement; osmotic diuresis from hyperglycemia; or with third spacing in conditions like pancreatitis or bowel obstruction. Then, there can be hypervolemic hyponatremia. This can occur when the serum sodium is diluted due to conditions like congestive heart failure, cirrhosis, or nephrotic syndrome. It can also happen in conditions where individuals are drinking too much water, called psychogenic polydipsia. Another condition is syndrome of inappropriate antidiuretic hormone secretion, or SIADH, where there is excess release of ADH, leading to water retention, which eventually dilutes sodium. All right, now clinical manifestations of hyponatremia are caused when fluid moves out of the extracellular space into the intracellular space. When this happens, common symptoms include nausea and vomiting, muscle cramps, fatigue, oliguria, and a rapid, weak pulse.