Diabetes insipidus: Nursing process (ADPIE)
1,679views
Diabetes insipidus: Nursing process (ADPIE)
Synthesis Of Nursing Practice
Synthesis Of Nursing Practice
Notes
| DIABETES INSIPIDUS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Harvey Nguyen is a 30-year-old male client who suffered a traumatic brain injury during a skiing accident 4 months ago.
He presents to his primary care physician, or PCP, with a report of increased thirst, increased urine output, and frequent nighttime urination.
He says he doesn’t go anywhere without a water bottle and always needs to know where the restroom is when he is away from home.
He says that he is tired all the time because he has to make frequent trips to the bathroom during the night.
His laboratory results are serum sodium 147 mEq/L; serum glucose 100 mg/dL; serum osmolality 312 mOsm/kg; urine specific gravity 1.001; and urine osmolality 248 mOsm/kg.
His PCP refers him to an endocrinologist who admits Harvey to the medical unit for a water deprivation test which confirms the diagnosis of central diabetes insipidus.
Diabetes insipidus is a condition characterized by excessive water loss through urine because the kidneys don’t reabsorb enough water.
Now, the primary hormone that regulates water reabsorption and balance in the body is ADH, also called vasopressin.
ADH is normally produced by the hypothalamus and is stored in the posterior pituitary, which are both located within the brain. To do this, the hypothalamus contains osmoreceptors, which are able to sense the osmolality of the blood.
The normal blood osmolality value is between 285 and 295 mOsm/kg. Now, when a person is dehydrated, osmolality increases, so osmoreceptors sense this and, in response, stimulate the pituitary to release the stored ADH into the blood.
ADH then travels to the kidneys to decrease water excretion in urine, and increase water reabsorption back into the blood, which ultimately helps restore normal blood osmolality.
In addition, osmoreceptors trigger the sensation of thirst. After the person drinks water, the osmolality returns to normal, and ADH secretion stops.
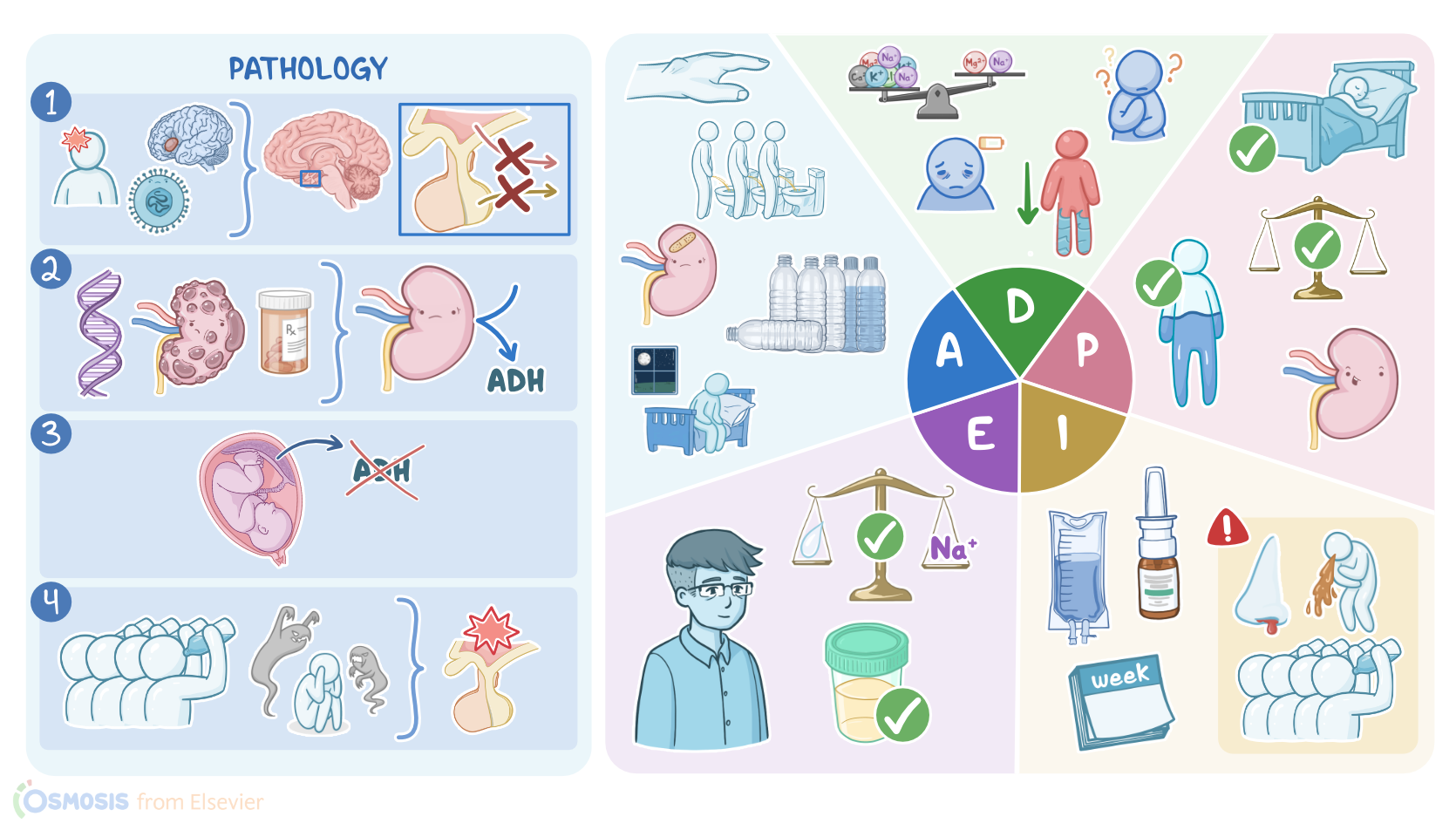
There are four types of diabetes insipidus. The first type is central diabetes insipidus, which is caused by a problem in the hypothalamus or pituitary gland, preventing ADH production or ADH release.
This can be due to a head injury, neurosurgery, brain tumor, vascular lesions like aneurysms, as well as due to an infection like meningitis or encephalitis, autoimmune conditions, or sometimes, the cause can be idiopathic.
The second type is nephrogenic diabetes insipidus, which is caused by a problem with the kidneys themselves, making them unresponsive to ADH.
This may be due to a genetic defect of the vasopressin receptors, or kidney disorders like polycystic kidney disease, as well as medications like lithium.
The third type is gestational diabetes insipidus, which occurs during pregnancy, because the placenta releases an enzyme called vasopressinase that breaks down ADH.
In other cases, pregnant clients generally produce more prostaglandins, which reduce kidney sensitivity to ADH.
Finally, the fourth type is dipsogenic diabetes insipidus, also called psychogenic or primary polydipsia, which is caused by drinking far too much water and it is often associated with a psychiatric disorder, such as schizophrenia, but can also be caused by damage to the hypothalamic osmoreceptors that regulate the feeling of thirst.
The most characteristic symptom of diabetes insipidus is that clients produce unusually large quantities of urine, which is called polyuria. A client with diabetes insipidus typically makes over 3 liters of dilute urine each day.
As a consequence, plasma osmolality increases, so osmoreceptors trigger thirst, causing the client to drink excessive amounts of water, which is called polydipsia.
Despite this, the kidneys remain unable to reabsorb water. As a result, diabetes insipidus can quickly lead to complications like dehydration, and low blood pressure. Clients may also develop electrolyte imbalances, such as hypernatremia or high blood sodium.
Now, acute hypernatremia causes neurological symptoms that range from lethargy, weakness, altered mental status, and irritability, to severe symptoms, like seizures and coma.
In addition, acute hypernatremia rapidly pulls water out of brain cells, so the brain as a whole shrinks. As a result, blood vessels within the brain may rupture and cause intracerebral and subarachnoid hemorrhages.
The diagnosis of diabetes insipidus typically starts with history and physical examination. In addition, a blood test would show an increased blood osmolality in central, nephrogenic, and gestational diabetes insipidus.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Diabetes Insipidus: New Concepts for Diagnosis" Neuroendocrinology (2020)
- "Diabetes insipidus related to sedation in the intensive care unit: A review of the literature" J Crit Care (2023)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Diabetes Insipidus: Pathogenesis, Diagnosis, and Clinical Management" Cureus (2021)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Diabetes Insipidus" Pediatr Rev (2020)