Dialysis care: Nursing
2,032views
Notes
| DIALYSIS CARE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| INDICATIONS |
| |
| TYPES OF DIALYSIS ACCESS |
| |
| PRINCIPLES OF DIALYSIS |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
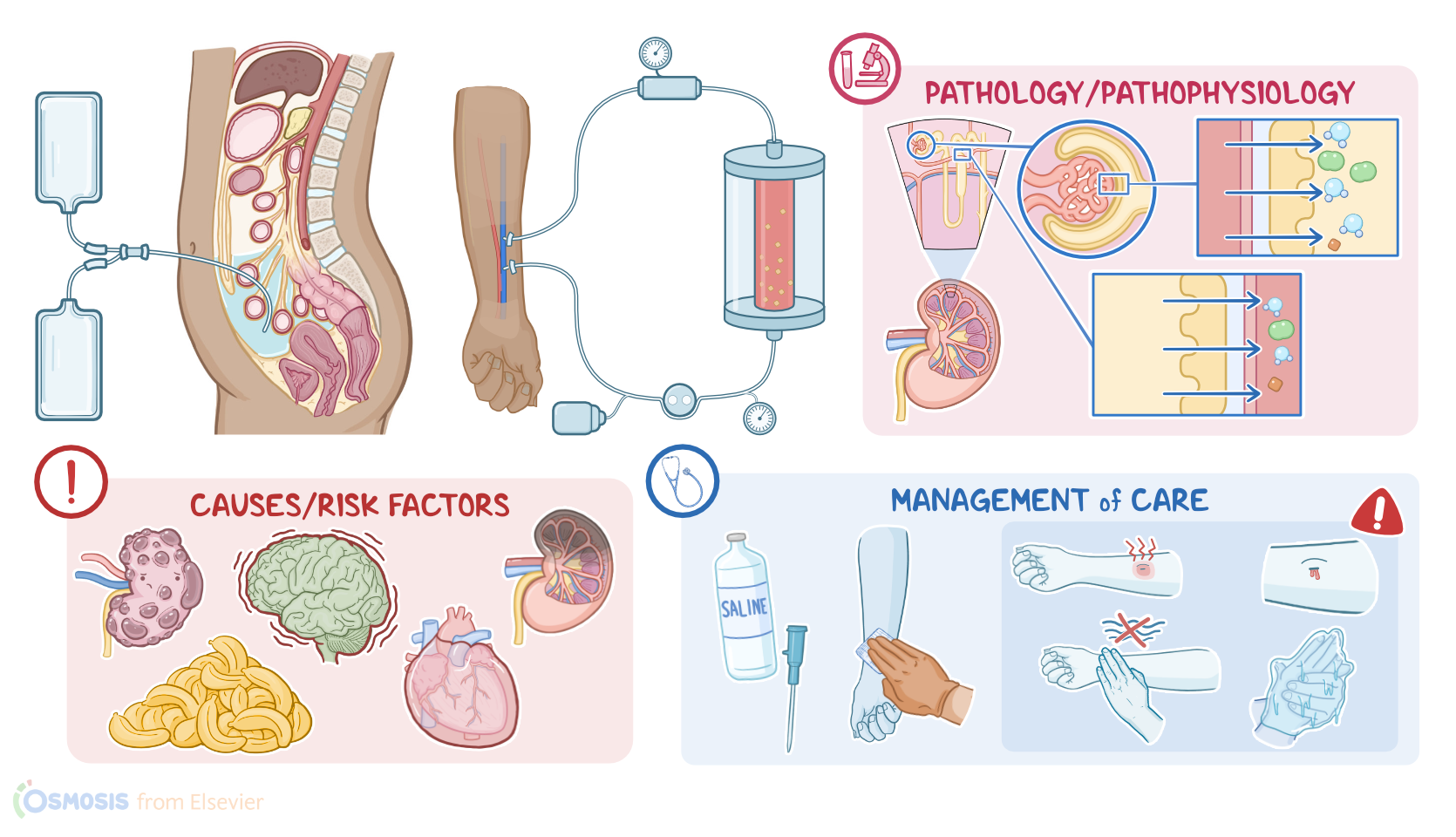
Dialysis is a type of kidney replacement therapy that removes toxic byproducts of protein metabolism, like urea, uric acid, and creatinine; waste products from the blood; as well as excess fluid. Additionally, through dialysis, electrolyte levels and acid-base imbalances can be corrected. There are two types of dialysis: hemodialysis and peritoneal dialysis. Now, let’s review some renal physiology. Each kidney is made up of millions of tiny functional units called nephrons, each of which consist of a renal corpuscle and the renal tubules. The renal corpuscle is where blood filtration happens, and it’s made up of the glomerulus, which is a tiny bundle of capillaries and the Bowman’s capsule, which is a cup-shaped structure surrounding the glomerulus. Blood flows through the glomerulus and then water and small solutes are filtered into Bowman’s capsule, creating an ultrafiltrate of blood. Then this ultrafiltrate goes through the renal tubules, where electrolytes and water can be secreted or reabsorbed.
In addition, they are important in regulating acid-base balance. The kidneys also clear blood of metabolic wasteful substances and toxins. Finally, what leaves the tubules becomes the urine, which flows into the bladder and is excreted during micturition. Okay, now, let’s look at some situations when dialysis is indicated. Most often, clients who require dialysis have end-stage chronic kidney disease, which means the kidneys have lost almost all their function. In this case, both hemodialysis and peritoneal dialysis are adequate long-term options. However, there are some urgent conditions that benefit from dialysis, and hemodialysis is usually preferred in these situations. These clients also usually have associated acute kidney injury.
Indications for urgent dialysis include pulmonary edema unresponsive to conventional treatment; life-threatening hyperkalemia, when potassium levels are over 6.5 mEq/L and there are associated electrocardiographic abnormalities; acidosis unresponsive to conventional treatment; signs of uremia, like encephalopathy or pericarditis; as well as intoxications, especially with methanol or ethylene glycol and certain medication overdoses, like lithium. Now, to perform dialysis on a client, first, you’ll need either vascular access for hemodialysis, or peritoneal access for peritoneal dialysis. Let’s start with hemodialysis, which requires venous access. In an acute setting, a temporary venous access is obtained through a temporary catheter in the subclavian, internal jugular or femoral vein. Clients on chronic hemodialysis need a more permanent access, such as an arterio-venous or AV fistula, where a connection between a small artery and a vein in the arm or less often the leg, is made surgically. Another semi-permanent access is a so-called permanent catheter that can be located in the same veins as the temporary catheter, but it can be used for a long time, is more comfortable for the client, and there’s a lower risk for infection than with the temporary access.
Finally, peritoneal access can be obtained by inserting a silicon rubber catheter in the peritoneal cavity Okay, now let’s look at the principles of dialysis, which are diffusion, osmosis, and ultrafiltration. Diffusion is the movement of solutes from a greater concentration to a lesser concentration until the two solutions have the same concentration of solutes. Osmosis is the health education platform that makes learning easy and fun, but in this case, it refers to the movement of fluid from an area of lesser solute concentration to an area of greater solute concentration. For example, glucose creates an osmotic gradient across the membrane and is able to pull excess fluid through that gradient. Finally, ultrafiltration refers to water and fluid removal according to a pressure gradient across the membrane, so water typically goes from where there’s more of it, like the body of a client with fluid overload, to where there’s less of it, like the other side of the dialysis membrane. Now, to understand how this works, let’s look at the dialysis machine. One of the most important components of the dialysis machine is the dialyzer, through which the client’s blood is filtered. The client will be connected to the dialysis machine using the venous access or the AV fistula using two tubules. One tubule will be responsible for taking the client’s blood and leading it to the dialyzer and the other one will return the filtered blood from the dialyzer.
The dialysis machine also has other important components, like the dialysate which is a type of solution used in the dialyzer to create a pressure gradient that makes diffusion happen. Other components include the blood pumps to help draw blood to the client, an arterial pressure monitor, an air trap or a sensor to detect air bubbles so that we can stop them from getting into the circulation. Finally, the dialysis machine also contains a heparin pump. That’s because anticoagulation is necessary during dialysis due to the risk of blood clots. In clients with a high risk for bleeding, a lower dose of heparin, citrate or no anticoagulation can be used. Finally, let’s look at peritoneal dialysis, which uses the peritoneal membrane as a dialyzer. Through the abdominal catheter, certain solutions can be introduced in the abdominal cavity and dwell in the peritoneal space for a certain amount of time, usually 4 hours. During this time, toxins are filtered through the peritoneal membrane. Afterwards, the fluid is drained and a new solution is introduced into the peritoneal cavity.
Okay, let’s look at the care you’ll provide for a client receiving hemodialysis. Your nursing priorities are to prepare your client for hemodialysis; monitor for complications, and provide psychosocial support. Now, to begin preparing your client for hemodialysis, check their pretreatment laboratory test results and assess their LOC, weight, heart and lung sounds. Also look for the presence of edema. When assessing their vital signs, remember to avoid checking their blood pressure in the extremity with the hemodialysis access site, and place a sign above your client’s bed alerting other care providers which limb has the access site. Then, closely examine their access site, checking for skin breakdown and infection; skin color and temperature; as well as capillary refill and pulses distal to the access site. If your client has an arteriovenous fistula or graft, also be sure to check the site’s patency by auscultating for a bruit, and palpating for a vibration or thrill. Immediately report signs of infection, such as redness, swelling, tenderness, or drainage; decreased pulses, sluggish capillary refill, or cool extremities; or if a bruit or thrill are absent. Then, prepare for additional assessment and interventions to support the function of the hemodialysis access site.