Disseminated intravascular coagulation (DIC): Nursing
Notes
| DISSEMINATED INTRAVASCULAR COAGULATION (DIC) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
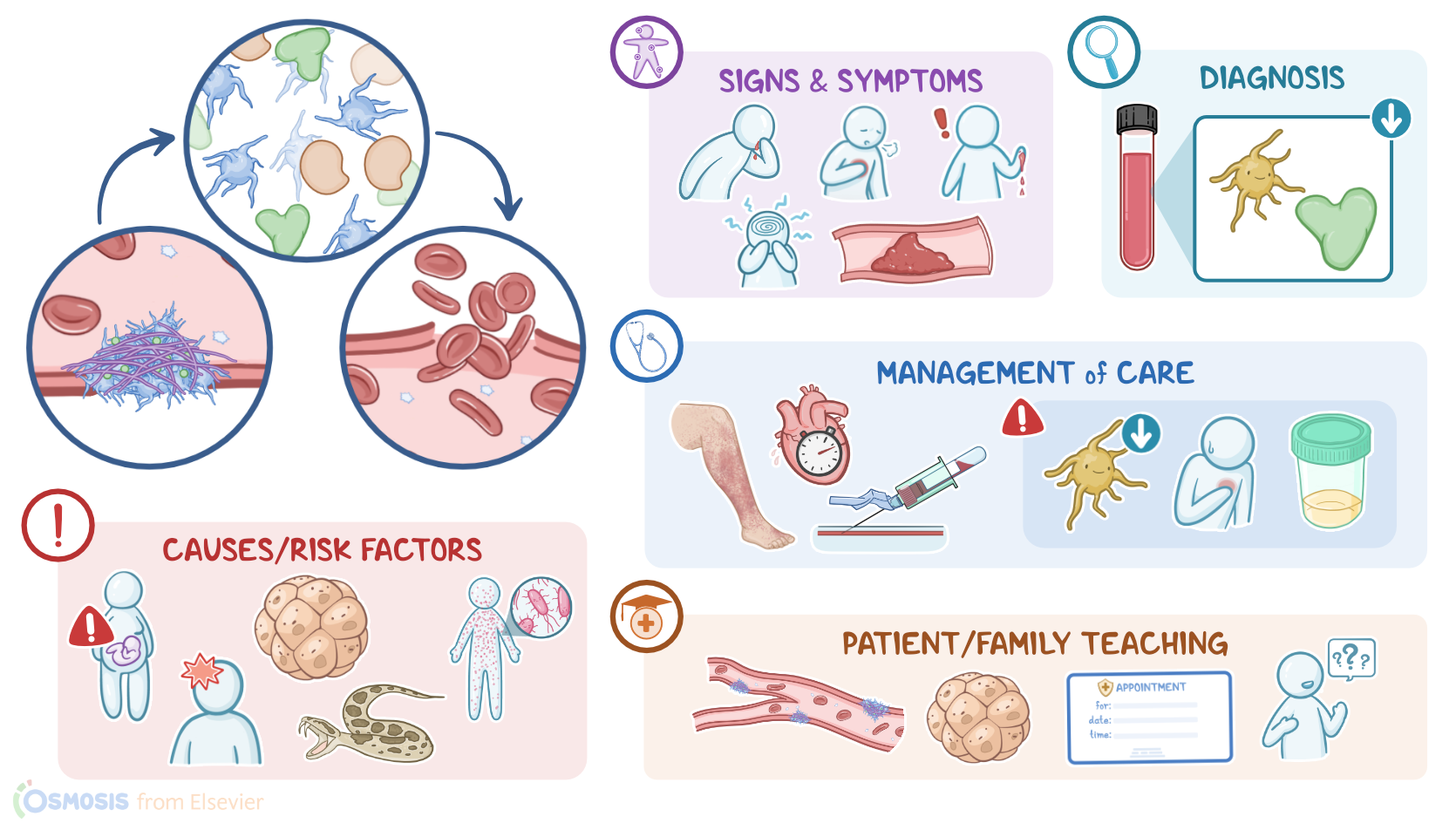
Disseminated intravascular coagulation, or DIC for short, is a rare but life-threatening condition. It is characterized by accelerated clotting within blood vessels, which in turn leads to increased consumption of platelets and clotting factors, which can ultimately result in uncontrollable bleeding.
Now, let’s quickly review the physiology of clotting, also known as the coagulation cascade, which is activated in response to an injury to limit the bleeding. So normally, when a tissue and its blood vessels are injured, the circulating platelets are activated locally and aggregate to form a temporary plug at the site of injury. The platelet plug then starts attracting circulating clotting factors, which starts off the coagulation cascade, ultimately resulting in the formation of fibrin, which in turn builds a tightly connected mesh that stabilizes the platelet plug. Lastly, in order to avoid excessive clotting, a protein called plasmin balances off the clotting process by breaking down the fibrin mesh and ultimately dissolving the clot through a process called fibrinolysis.
Now, DIC is caused by the presence of an underlying disorder that triggers uncontrolled activation of the coagulation cascade.
The most common cause is sepsis. Other causes include cancer, serious trauma, and obstetric complications, such as a placental abruption or amniotic fluid embolism.
In addition, DIC can be caused by a severe immune reaction, which can be triggered by an incompatible blood transfusion, organ transplant rejection, or toxins like snake or spider venom.
Now, the pathology of DIC develops when a severe disorder or immune reaction triggers massive systemic activation of the coagulation cascade, resulting in widespread clot formation intravascularly, hence the name disseminated intravascular coagulation. These clots can then go on and block small and midsize vessels, causing ischemia or necrosis of the involved tissue. Additionally, this widespread clotting leads to increased consumption of platelets and clotting factors. As a result, clients are at risk of uncontrollable and life-threatening bleeding, even from minor injuries, like venipuncture sites.
Alright, so the first clinical manifestations of DIC often include undue bleeding from the nose, gums, or mouth; as well as blood in the stools due to gastrointestinal bleeding; blood in the urine due to urinary tract bleeding; visual changes due to retinal hemorrhage; or simply blood oozing from puncture sites. More severe manifestations of deep tissue bleeding include altered mental status, chest pain, and dyspnea, along with palpitations, tachycardia, and even shock.
Additionally, clients can present with clinical manifestations from clotting. These include venous thromboembolism, such as deep vein thrombosis, where the obstructed venous flow in the legs may present with leg pain and swelling. Another manifestation can be arterial thrombosis, which can cause ischemia and even necrosis of the involved organ. Other findings may include bluish discoloration of nail beds and lips due to cyanosis; as well as complications like myocardial infarction or stroke. Ultimately, the combination of bleeding and ischemia may result in organ hypoperfusion, which may even lead to multi-organ failure.
The diagnosis of DIC starts with the client’s history and physical assessment, followed by laboratory tests. Typical laboratory findings in DIC include a CBC that shows a decreased platelet count; decreased fibrinogen level; as well as a prolonged prothrombin time or PT, and prolonged partial thromboplastin time or PTT, both of which reflect decreased levels of circulating clotting factors. In addition, there’s an elevated level of D-dimer, which is a fibrin degradation product, indicating significant blood clot formation and subsequent fibrinolysis.
Treatment of DIC involves supportive measures, including IV fluids and blood products to replace the blood loss; as well as anticoagulant medications to counteract excessive clotting; and ventilator support in cases of respiratory failure. Definitive treatment of DIC focuses on addressing the underlying cause, when possible.
Okay, let’s look at the nursing care you’ll provide for a client with DIC. Your priorities of care are to decrease bleeding, monitor for abnormal clotting, and address the underlying cause.
Sources
- "McCance & Huether’s pathophysiology: The biological basis for disease in adults and children (9th ed.). ISBN: 978-0-323-78987-5 " Elsevier (2023)
- "Lewis’s medical-surgical Nursing (12th ed.) ISBN:978-0-323-78961-5 " Elsevier (2023)