Epididymitis: Nursing
Epididymitis: Nursing
Medical Surgical
Medical Surgical
Notes
| EPIDIDYMITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Epididymitis is an inflammation of the epididymis that most commonly affects young, sexually active clients assigned male at birth under 35 years of age. It is usually characterized by unilateral pain and swelling in the scrotum. First, let’s recall the anatomy and physiology of the epididymis, which is a tubular, comma-shaped structure curving superiorly and posteriorly around the testes. The epididymis collects and stores the sperm cells produced by the testicle until they are mature and capable of fertilization. During ejaculation, sperm leave the epididymis and travel via ductus, or vas deferens, to the prostate gland, where it enters the urethra to be expelled outside of the body. The urethra is also the way urine is excreted from the body, but during ejaculation, the bladder sphincter right above the prostate contracts and prevents urine from mixing with sperm.
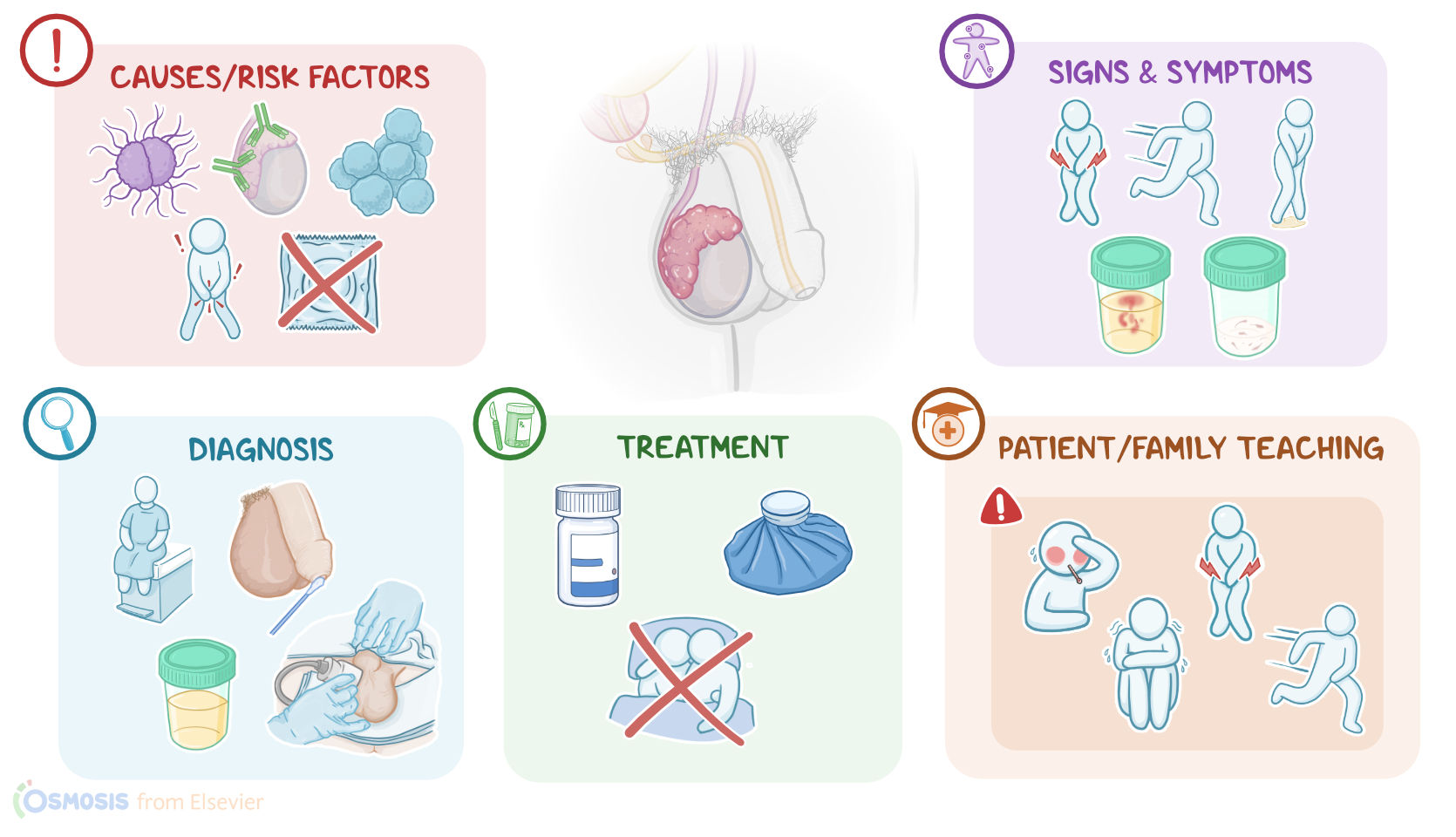
Now, the causes of epididymitis often vary with age. The most common cause of epididymitis in clients younger than 35 is a sexually transmited infection or STI, especially from bacteria like Neisseria gonorrhoeae and Chlamydia trachomatis. The most common cause of epididymitis in older clients and children, is an urinary tract infection or UTI with bacteria from the gastrointestinal tract, such as Escherichia coli. Less common causes of epididymitis include; viruses, such as mumps virus, as well as non-infectious causes, including trauma and irritation, medications like amiodarone, and autoimmune disease.In addition, there are also certain risk factors for developing epididymitis. Non-modifiable risk factors include being aged 20 to 39 years old and having congenital abnormalities of the genitourinary tract. Modifiable risk factors, on the other hand, include increased sexual activity, multiple sexual partners, and anal or unprotected intercourse. Other modifiable risk factors include urinary retention, which could be due to benign prostatic hyperplasia, or prostatitis; as well as engaging in sports with repetitive motions like jumping or running, and exercising or having sexual intercourse with a full bladder.
Moving on to the pathology of epididymitis, the bacteria usually start by colonizing the urethra, then make their way to the prostate, and further down the vas deferens, and finally, invade the epididymis. Additionally, obstruction of urine flow at the level of the prostate leads to urine retention, and even backflow of urine, or urinary reflux. This way urine may enter the vas deferens and carry bacteria down to the epididymis. Rarely, the epididymis can get infected via spread through the bloodstream, usually as a consequence of bacteremia or viremia. Once the pathogen reaches the epididymis, they usually trigger an inflammatory response, which is characterized by increased blood flow, vasodilation, and swelling. At the same time, white blood cells get attracted to fight off the infection.Now, complications of epididymitis include epididymal abscess formation, and involvement of the testes leading to epididymo-orchitis. This may also result in testicular abscess formation, and in severe cases, sepsis. Additionally, inflammation of the epididymis may lead to scarring and fibrosis, and subsequently, infertility, or even sterility if both epididymides are involved.
Clinical manifestations of epididymitis typically include unilateral localized testicular pain that might radiate to the lower abdomen. This can be accompanied by urinary symptoms, such as dysuria, urinary frequency and urgency, as well as urinary incontinence. Rarely, clients can present with purulent urethral discharge, hematuria, hematospermia, fever and chills in case of sepsis. Upon physical assessment, there is typically swelling and tenderness along the superior and posterior aspect of the testis. Scrotal skin can also be erythematous, warm and indurated. Additionally, regional inguinal lymph nodes are commonly tender and enlarged.In clients with prostatitis, digital rectal examination may also reveal tenderness of the prostate gland. Diagnosis of epididymitis usually begins with the client's history and physical assessment, followed by urinalysis, which usually shows hematuria and pyuria. A urethral swab or urine culture can be performed to identify the causative pathogen. In addition, imaging tests can be done, most commonly ultrasound, which may show increased blood flow and thickening of the epididymis.