Glomerulonephritis: Nursing
1,704views
Glomerulonephritis: Nursing
Watch later
Watch later
Notes
| GLOMERULONEPHRITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Glomerulonephritis refers to inflammation of the glomeruli. It can be primary when the disease starts in the glomeruli, or secondary, when the glomeruli are affected by systemic disease. It can also be acute, when symptoms develop suddenly and resolve with treatment; or it can be chronic if acute disease is not treated, or when the disease process develops slowly, leading to irreversible failure of the kidneys.
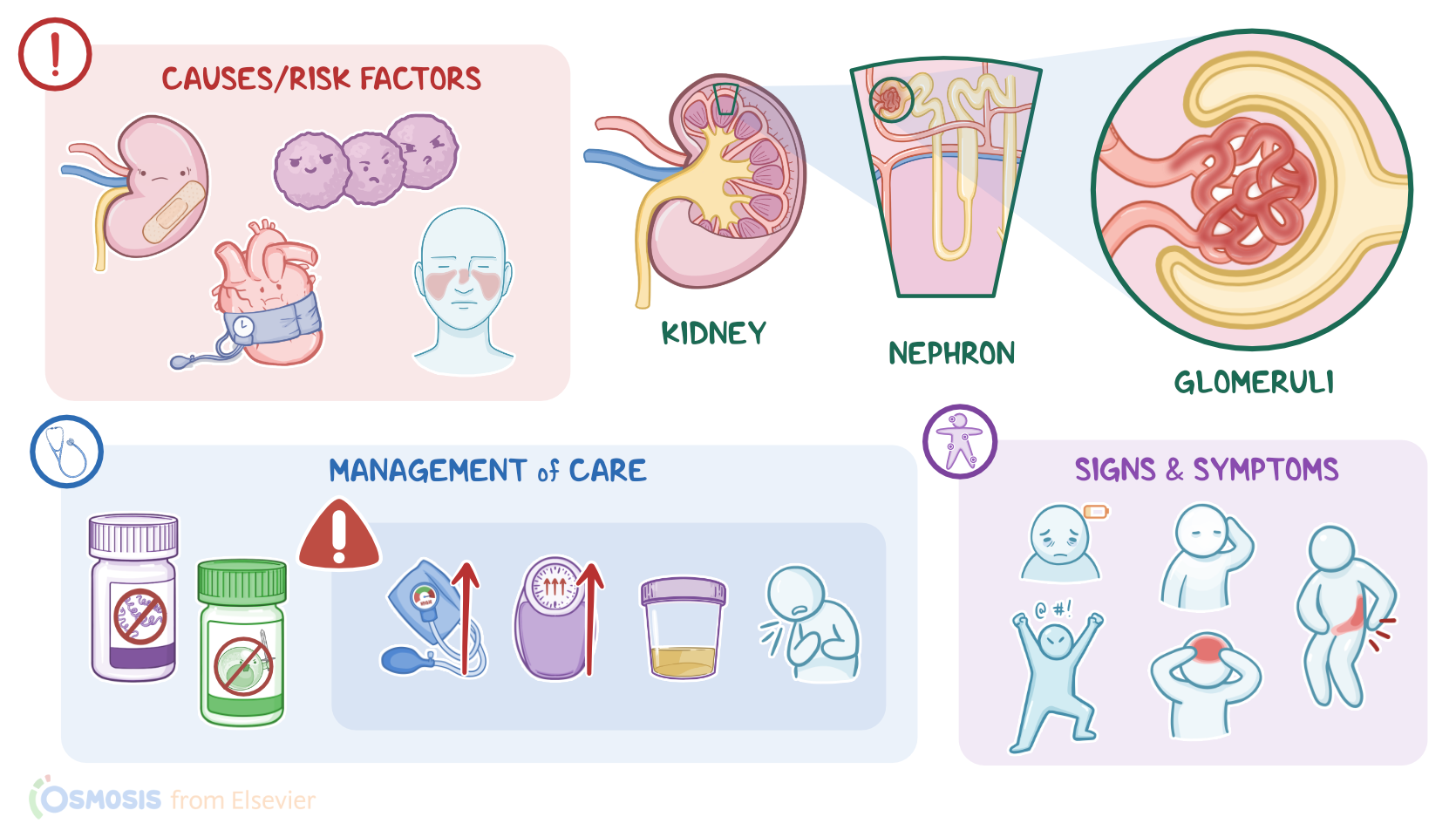
First, let’s quickly review some kidney physiology! Remember that the nephron is the functional unit of the kidney, and its role is to filter waste products and water from the blood. Each nephron is made up of a renal corpuscle and a set of renal tubules, which are, in order: the proximal convoluted tubule, loop of Henle, distal convoluted tubule and finally, collecting ducts which drain urine into the renal papillae and eventually empty into the renal pelvis.
The renal corpuscle is made up of the glomerulus, which is a bundle of capillary loops, and Bowman’s capsule, which surrounds the glomerulus. Now, blood enters the glomerulus through the afferent arteriole, then moves inside the glomerulus, where glomerular filtration occurs. Then, the remaining blood exits the glomerulus through the efferent arteriole. Now, the glomerular capillary wall is a semi-permeable membrane with three layers: the endothelium, which is the inner layer; the basement membrane; and the epithelium, which is the outermost layer.
For filtration to occur, the endothelial and epithelial cells that line the capillary wall are separated by small pores that filter water and small particles from the blood and into the Bowman capsule. Only small particles are filtered from the blood and never proteins, since they are larger molecules. Also, normally, there aren’t any red blood cells in the urine. For glomerular filtration to occur, the hydrostatic pressure created by the blood pressure needs to be greater than opposing forces, such as the tubular filtrate and oncotic pressure, which is the pressure of proteins. The final product of filtration is called filtrate or primary urine, which will flow through the Bowman capsule into the proximal convoluted tubule.
Now let’s look at the causes of glomerulonephritis. Causes and risk factors of acute primary glomerulonephritis include infections with various agents. Some bacteria that can cause acute primary glomerulonephritis include, Group A beta-hemolytic Streptococcus, which is the most frequent in children; but also Streptococcus pneumoniae, Klebsiella pneumoniae, Mycoplasma pneumoniae, and Treponema pallidum, which causes syphilis; as well as staphylococcal or gram negative bacteremia or sepsis. There are also viruses that can cause acute primary glomerulonephritis which include dengue fever virus, hantavirus, varicella, parvovirus, hepatitis B and C viruses, cytomegalovirus, Epstein-Barr virus and human immunodeficiency virus.
Next, acute secondary glomerulonephritis can be caused by systemic conditions, like systemic lupus erythematosus, amyloidosis, chronic liver conditions like hepatitis B and C, autoimmune hepatitis, or cirrhosis, as well as other conditions, like vasculitis, Goodpasture syndrome, diabetic nephropathy and HIV-associated glomerulonephritis. Now, when it comes to chronic glomerulonephritis, sometimes the causative agent isn’t known, but infections, untreated hypertension, immunological injuries to the kidneys, inflammation or impaired renal perfusion can all lead to chronic glomerulonephritis over time.
Now, let’s delve into the pathology of glomerulonephritis. With acute glomerulonephritis, infections or systemic conditions cause an excessive immune response in the kidneys. This leads to inflammation and injury in the glomerular basement membrane, which impairs glomerular filtration, so blood and proteins can make it through the filtration barrier and into the urine.
Acute poststreptococcal glomerulonephritis, develops about 1 to 2 weeks following an infection with nephrotoxic strains of group A beta-hemolytic streptococci. This can be a skin infection like impetigo or a throat infection of the tonsils or pharynx. After the infection, antibodies against the streptococcal antigen are made. Then antigen-antibody complexes are formed and deposited in the glomeruli leading to activation of the complement system. This further leads to inflammation and then acute kidney injury.
With chronic glomerulonephritis, kidney tissue gradually atrophies and the number of nephrons decreases, which leads to reduced glomerular filtration, sclerosis in the renal arteries, and a decline in renal function. If a biopsy is done in the late stages of chronic glomerulonephritis, there’s cell loss, protein and collagen deposits and fibrosis in the kidney tissue. Glomerulonephritis can lead to other problems such as nephrotic syndrome or eventually lead to end-stage renal disease.
Now let’s look at the clinical manifestations of glomerulonephritis. General manifestations include lethargy, irritability, pallor and headaches. The client can also have abdominal or flank pain, as well as nausea, vomiting, and anorexia. There can also be periorbital edema, generalized edema, or even pulmonary edema, which could present as dyspnea. Urinary manifestations can include decreased urine output, dysuria, and hematuria, which could turn the urine tea or cola colored, with a cloudy, smoky aspect. Mild to moderate hypertension is also often present.
Diagnosis of glomerulonephritis starts with the client’s history and physical assessment. Urinalysis shows hematuria and proteinuria. Microscopic examination of the urine usually shows dysmorphic erythrocytes and red blood cell casts, along with epithelial casts. A 24 hour urine collection can be done in order to quantify the protein excretion rate, which is increased, ranging from 500 milligrams to 3 grams per 24 hours.
With both acute and chronic glomerulonephritis, there can be elevated creatinine and BUN levels, which is called uremia. Then an estimated glomerular filtration rate is calculated based on creatinine levels. A serum electrolyte panel, along with an acid-base status can also show abnormalities. With acute poststreptococcal glomerulonephritis, there’s an increased titer of anti-streptolysin O antibodies, and complement fractions like C3 and C4 can be lower than normal. Finally, to identify the cause of glomerulonephritis, an immunological panel, along with a kidney biopsy can be performed. Additionally, a CT-scan of the abdomen can be done to identify structural abnormalities of the kidneys.