Herniated intervertebral disc: Nursing
Notes
| HERNIATED INTERVERTEBRAL DISC | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
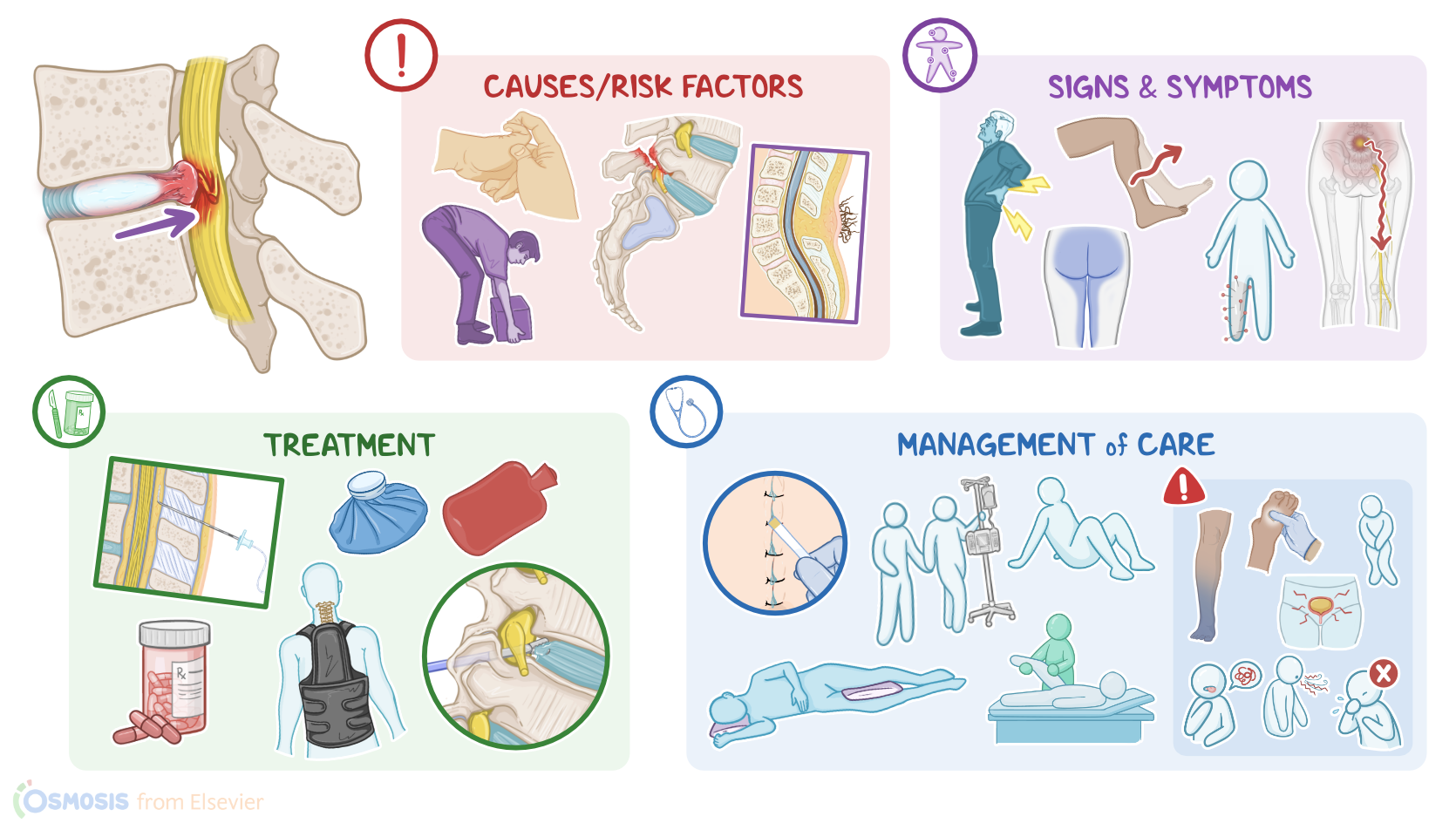
| CAUSES AND RISK FACTORS |
| |
| PATHOLOGY |
| |
| CLINICAL MANIFESTATIONS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Content Reviewers
A herniated intervertebral disc refers to a bulging or protrusion of part of the intervertebral disc, which is rubbery cushion between the vertebrae of the spine. Herniated intervertebral discs are one of the most common causes of back pain.
First, let’s quickly review some anatomy and physiology. The bony spine, also known as the vertebral column, consists of 33 vertebrae that provide support for the head and protect the spinal cord. Between the vertebrae are the intervertebral discs, which are fibrocartilaginous structures that provide stability, allow spinal motion, and absorb shocks along the spinal column.
They have a central part called the nucleus pulposus, which is composed mostly of water, but also proteoglycans and some collagen. It provides volume for the disc, absorbs shock, and helps distribute weight and pressure evenly between the vertebrae. The tougher, outer part is called the annulus fibrosus, which is composed mostly of collagen fibers, but also some water and proteoglycans. It provides stability and protects the central nucleus pulposus.
Finally, there’s an anterior longitudinal ligament, which runs down the anterior surface of the vertebrae, and a posterior longitudinal ligament, which is much narrower and attached to the posterior surface of the vertebral bodies, and the intervertebral bodies.
Now, the spinal cord travels through the spinal canal and stops at the second lumbar vertebra. Here it ends in a cone, called conus medullaris. Since the spinal cord is shorter than the spinal canal, the nerves of the lumbar, sacral, and coccygeal regions have to travel down the spinal canal to reach their corresponding openings. In doing so, they form a nerve bundle below the spinal cord called the cauda equina.
Now, the main cause for herniated discs seems to be the daily stress applied to the spine throughout a client’s lifetime. Less commonly, herniated intervertebral discs can be caused by spinal trauma, connective tissue disorders, such as Ehlers-Danlos syndrome, and congenital defects of vertebral formation.
So, important risk factors for herniated discs include non-modifiable ones, such as age, especially 30 to 50 years; being assigned male at birth, and family history of herniated discs, alongside modifiable ones, like obesity, spine overuse, or injury due to excessive physical activity, and smoking.
Now, the pathology of herniated discs occurs when the intervertebral disc wears away from repetitive stress, becoming weaker and losing elasticity and flexibility.
So, the nucleus pulposus loses its shock-absorbing capacity, and cannot evenly distribute the weight and pressure among the vertebrae. This shifts the weight and pressure on the less elastic annulus fibrosus, causing wear and tear injuries that accumulate over time.
These injuries weaken the structure of the annulus fibrosus, so the nucleus pulposus starts pushing against it, causing it to bulge outwards, which is referred to as disc protrusion. If the annulus fibrosus gets torn at this site, the nucleus can slip out and lead to disc herniation.
Intervertebral disc herniation most commonly occurs unilaterally and posterolaterally, since this is a weak point that is not supported by the posterior longitudinal ligament. The disc bulges into the spinal canal and may compress the root of the local spinal nerve against the lamina of the vertebrae. This leads to irritation and inflammation of the nerve root, which is known as radiculopathy. Less commonly the herniation can develop posteriorly, where the bulging disc compresses the spinal cord directly, causing myelopathy.
Now, parts of the spine that are the most mobile put more stress on their intervertebral discs. Therefore, the lumbar spine is the most common site of disc herniation, especially at the levels of L4-L5 and L5-S1, followed by the cervical spine, especially C5-C6 and C6-C7. The thoracic spine, on the other hand, is the least mobile and rarely affected by disc herniation, but when it does occur, it is most common at the T11-12 levels.
Now, complications of intervertebral disc herniation may develop when the compression is severe or is left untreated. These include chronic back pain and permanent nerve damage.
Finally, herniations at the lumbar region can compress on the nerves of the cauda equina, leading to what’s known as cauda equina syndrome.
This is characterized by severe lower back pain and decreased bowel and bladder control, as well as sexual dysfunction. It can also cause saddle anesthesia, which is a loss of sensation in the saddle area, which includes the buttocks, inner surface of the thigh, and perineum.
Also, one or both legs can be impaired by muscle weakness, loss of knee and ankle reflexes, and even paraplegia.
The cauda equina syndrome is considered a medical emergency since emergent surgical decompression is usually needed in order to prevent permanent nerve damage.
Clinical manifestations mainly depend on the location of the herniated intervertebral disc and the extent of spinal nerve root compression. In general, there is a sharp or burning pain, along with motor or sensory loss along the field of innervation of the affected nerve.
So, starting from the cervical spine, in radiculopathies for all C5, C6, C7, and C8 nerve roots, the pain radiates into the shoulder, pectoral and scapular regions, down the arm, and to the hand. Clients may also experience weakness in shoulder movement and handgrip, as well as paresthesia.
Reflexes might also be reduced or absent. So C5 radiculopathy affects the biceps and brachioradialis reflexes, while C7 radiculopathy affects the triceps reflex.
Moving on to the thoracic spine, thoracic disc herniations can cause axial back and chest pain. Thoracic radiculopathies can also cause band-like chest or abdominal pain that radiates along the area innervated by the affected intercostal nerve. Herniations at the lower level of the thoracic spine may even cause bowel, bladder, and sexual dysfunction.
Continuing down to the lumbar spine, a key symptom of lumbar disc herniation is sciatica or a shocking pain that shoots down from the buttocks through the leg, following the course of the sciatic nerve. Some clinical manifestations include walking in a stiff and flexed position due to severe back pain, or clients might not be able to bend at all.
In L4 radiculopathy, there are also motor deficits like weakness in knee extension and reduced patellar reflex. On the other hand, in L5 radiculopathy, the motor deficits include weakened hip abduction and weakened foot dorsiflexion.
Clients with L4 or L5 radiculopathy typically limp while walking and may have difficulty in heel walking.
Lastly, clients with S1 radiculopathy may present with weakened foot plantar flexion and a diminished Achilles tendon reflex, as well as difficulty in toe walking.
On the other hand, S2 to S4 radiculopathies lead to sensory loss of the perineal and perianal regions and on the medial buttock area.
Radiculopathies of the S2 to S4 also affect the bulbocavernosus reflex, where squeezing the glans of the penis or clitoris, can not produce anal sphincter contraction.
The anal wink reflex might be absent as well, meaning that scratching the skin of the perineum and around the anus does not produce anal sphincter contraction either.
Okay, diagnosis of the intervertebral disc herniation starts with the client’s history and physical assessment. Imaging studies like X-ray may show signs of degenerative disc disease like loss of vertebral height, while an MRI of the spine can confirm the diagnosis. Electromyography, or EMG, of the extremities, might also be useful in assessing the severity of nerve irritation.
A common test used in diagnosing lumbar disc herniation is the straight leg raise test, or SLR, where a client laying on their back keeps their legs straight and then raises them one at a time between 30 and 60 degrees. If they experience pain radiating down their leg, the test is considered positive, suggesting lumbar disc herniation.
Additionally, a myelography could be performed, where contrast is injected into the spinal canal for better visualization of the spinal cord and other structures.