Hyperosmolar hyperglycemic state (HHS): Nursing process (ADPIE)
Hyperosmolar hyperglycemic state (HHS): Nursing process (ADPIE)
Watch later
Watch later
Notes
| HYPEROSMOLAR HYPERGLYCEMIC STATE (HHS) | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Malcolm Johnson is a 68-year-old male client with a history of poorly controlled type 2 diabetes mellitus who recently recovered from viral pneumonia.
Over the past few days, he has felt more thirsty than usual, has been urinating frequently, and has felt fatigued.
This morning his son, Kyrone, noticed his father seemed confused, so he checked Mr. Johnson’s blood sugar and the reading was 685 mg/dL.
Kyrone promptly brought Mr. Johnson to the emergency department. Lab results revealed elevated serum glucose, elevated serum osmolarity, and negative serum ketones.
Mr. Johnson is being admitted to the medical intensive care unit for hyperosmolar hyperglycemic state.
Hyperosmolar hyperglycemic state, or HHS for short, is a metabolic complication of diabetes mellitus, more often in type 2 than type 1 diabetes.
HHS occurs when the blood glucose levels go really high, over 600 mg/dL, which leads to extremely increased urination, or polyuria.
This ultimately causes severe dehydration, resulting in a blood osmolarity of over 320 mOsm/kg.
Now, osmolality is the concentration of dissolved particles in the blood, and one of the major particles is glucose.
Normally, blood glucose levels should be lower than 100 mg/dL while fasting for over 8 hours, and lower than 140 mg/dL 2 hours after eating; so normal blood osmolality is maintained between 285 and 295 mOsm/kg.
Glucose is a polar molecule, which means it cannot passively diffuse across cell membranes, so it needs insulin to regulate its membrane transport into the cells.
As a consequence, when it is increased, it remains in the blood vessels and causes a hyperosmolar state that draws water into the blood.
As a result, water begins to leave the body’s cells and enter the blood vessels, leaving the cells relatively dry and shriveled.
The excess of water within blood vessels is eliminated via urination, which leads to polyuria and severe total body dehydration.
Now, HHS mainly occurs in clients with uncontrolled type 2 diabetes, leading to hyperglycemia,
There’s a higher risk of HHS in older clients, especially those with impaired cognitive function or thirst perception, as well as those who do not adhere to their treatment regimen for diabetes.
Other risk factors include acute conditions, such as an infection, a stroke, or myocardial infarction.
Finally, there’s increased risk of HHS among clients who take medications like glucocorticoids, which impair glucose tolerance, or diuretics, which increase urination, as well as having surgery, which puts the body under metabolic stress.
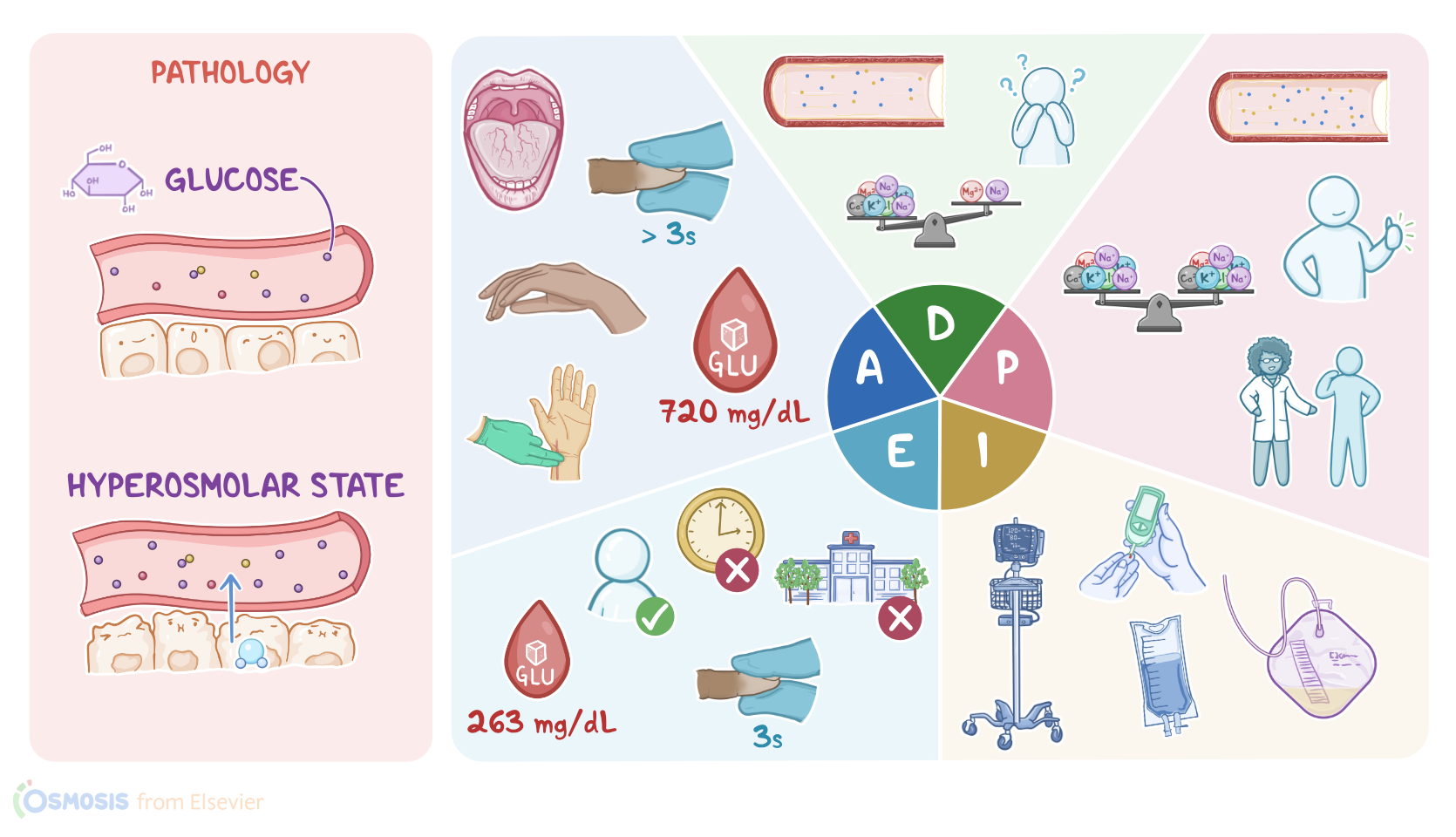
Okay, now HHS typically presents with polyuria associated with symptoms of severe dehydration, like extreme thirst, dry mouth, decreased skin turgor, anhidrosis or decreased sweating, and poor capillary refill. In addition, clients may develop hypotension and tachycardia.
If not promptly treated, severe dehydration can affect the brain, causing neurological symptoms that range from lethargy, weakness, confusion, and hallucinations, to severe complications, like seizures, and may quickly deteriorate to cerebral edema, potentially leading to coma.
Other complications of HHS include myocardial infarction, stroke, and even death.Okay, now the diagnosis of HHS typically starts with history and physical examination.
In addition, a blood test would show severe hyperglycemia and an increased blood osmolality. BUN and creatinine are also markedly elevated.
On the other hand, electrolytes like sodium and potassium can be decreased, and there’s usually no acidosis, and no or minimal ketone bodies in urine.
Treatment of HHS includes aggressive IV fluids and electrolyte replacement, followed by IV insulin to reduce glucose levels.
Okay, you’re ready to begin Mr. Johnson’s assessment. Mr. Johnson appears fatigued with sunken eyes and is looking around the room asking where he is.
His oral mucous membranes are dry; he has warm, dry skin with poor turgor; capillary refill is more than 3 seconds.