Increased intracranial pressure (ICP): Nursing
2,611views
Increased intracranial pressure (ICP): Nursing
Final Exam Prep Playlist
Final Exam Prep Playlist
Notes
| INCREASED INTRACRANIAL PRESSURE (ICP) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
Transcript
Increased intracranial pressure is a potentially life-threatening condition characterized by increased pressure within the skull.
First, let’s take a look at the physiology of intracranial pressure or ICP, which is how much pressure there is within the cranium and spinal column, and it plays an important role in how much oxygen gets to the brain. ICP, which is normally between 7 and 15 mmHg, is determined by the cerebral perfusion pressure or CPP, which is the amount of force available to deliver blood to the brain. CPP is defined as the difference between the mean arterial pressure, or MAP and the ICP.
Now, when it comes to regulating ICP, remember that the mature skull is a rigid structure that can’t expand. So, to maintain a normal ICP, there must be a balance between the volumes of its contents, including brain tissue, cerebrospinal fluid or CSF, and blood supplying the brain. As a result, if there’s an increase in the volume of any one of these three, there should be a compensatory decrease in the other two, which is known as the Monroe-Kellie hypothesis. Normally, the volume of the brain remains relatively stable, so ICP can be regulated by changes in CSF and blood volume. When needed, CSF production can be decreased or reabsorption can be increased to help bring ICP back to normal. Similarly, cerebral blood volume can be decreased either by cerebral vasoconstriction or increasing the venous blood drainage out of the skull.
Finally, it’s worth noting that cerebral blood vessels are lined by highly selective endothelial cells that only allow certain substances to pass into the interstitial fluid surrounding the neurons. This is commonly referred to as the blood-brain barrier, and it helps protect the neurons from pathogens, some immune cells, different products of metabolism as well as some medications that can be found in the systemic circulation.
So, increased ICP can be caused by an increased volume within the skull. An increase in brain tissue volume might develop in the case of cerebral edema, which is an excessive buildup of fluid throughout the brain tissue. Some causes of cerebral edema include encephalitis, hyponatremia, and a large ischemic stroke. In addition, space-occupying lesions such as brain tumors or abscesses, as well as intracranial hemorrhage, can also lead to increased ICP. Finally, increased ICP may be caused by increased CSF production, like in a choroid plexus tumor; as well as impaired CSF circulation, like in obstructive hydrocephalus; or decreased CSF reabsorption, like in meningitis or a subarachnoid hemorrhage.
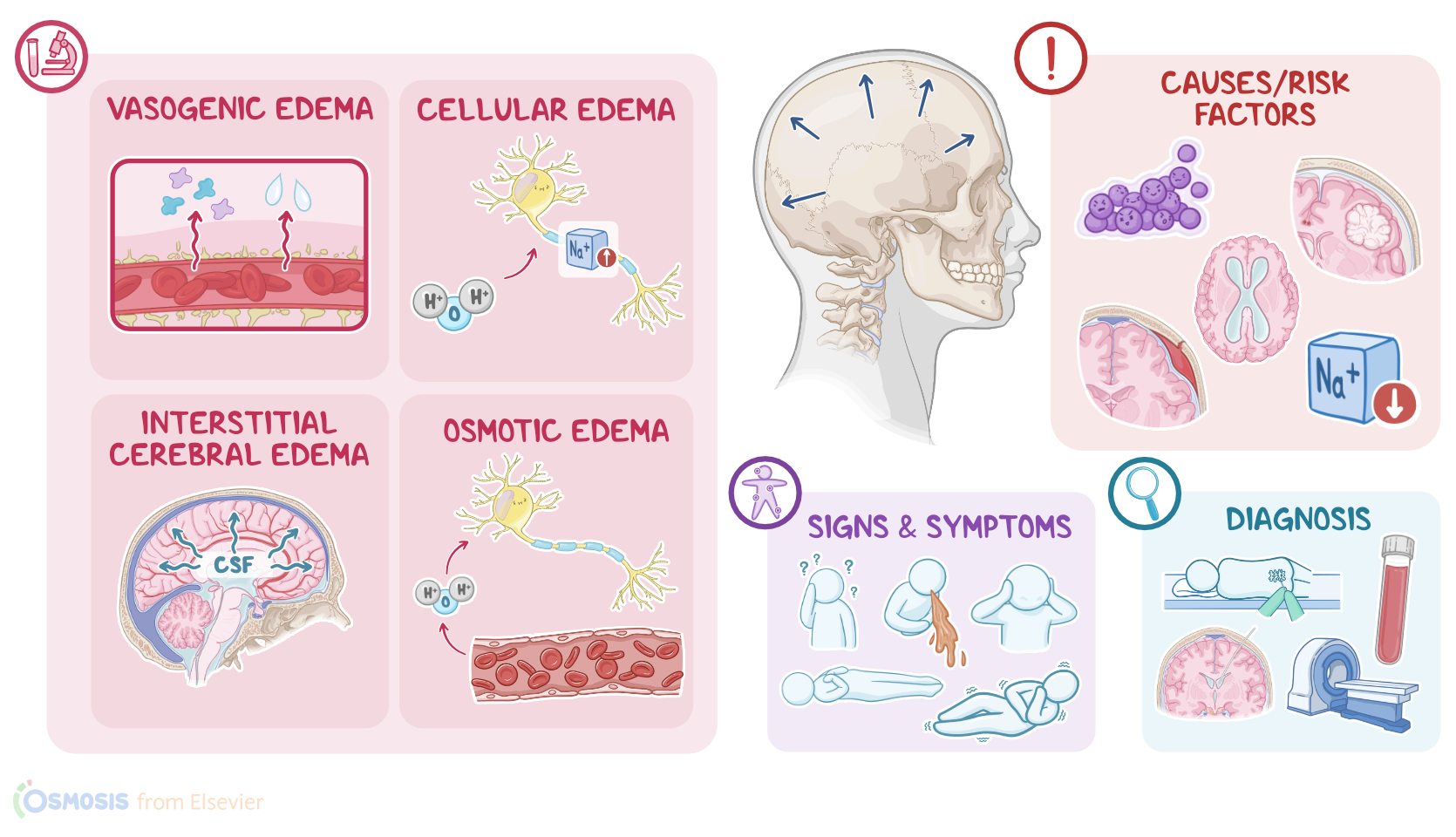
Now, when it comes to pathology, there are 4 major causes of cerebral edema. First up, there’s vasogenic edema, which is the most common form, and it’s when the blood-brain barrier is disrupted, allowing more molecules, like proteins, to pass out of the blood vessel and into the interstitium. In turn, this creates an increased osmotic pressure that draws fluid into the brain interstitium, increasing the ICP.
Second, there’s cellular edema, also known as cytotoxic edema. In this case, injury to the brain cells causes an increase in intracellular sodium, which, in turn, makes more water enter the cells. So increased ICP is on account of the cells swelling up with water.
Third, there’s interstitial cerebral edema, which is when CSF flows from the brain ventricles into the interstitium.
And finally, there’s osmotic edema, which is when disturbances in the osmotic pressure in the blood, such as hyponatremia, makes brain cells pull in water from the blood, which increases the ICP.
Now, the compensatory mechanisms that keep ICP within a normal range have limits, and can be overwhelmed. When this happens, ICP starts to increase, which puts pressure on the ventricles and cerebral blood vessels. In turn, this decreases cerebral blood flow and cerebral perfusion. Lower cerebral perfusion means that less oxygen is delivered to the brain tissue, which causes neurons to swell up and die, worsening the already increased ICP. At the same time, carbon dioxide starts building up, causing vasodilation, which allows even more fluid to leak from the blood vessels into the brain tissue.
If not corrected, increased ICP can lead to complications, such as papilledema, which is the swelling of the optic disc, which is the point where the optic nerve leaves the retina. The most severe complication, though, is brain herniation. Brain herniation occurs when a part of the brain is pushed into another space of the skull or even out of it, and this can affect other CNS structures, like the brainstem. Brain herniation can either be supratentorial and infratentorial. Supratentorial herniation refers to displacement of the cerebrum above the tentorium, which is a meningeal fold located in the back of our skull that separates the cerebrum from the cerebellum. Infratentorial herniation refers to herniation of the cerebellum, which is located below the tentorium.