Intestinal obstruction: Nursing
Notes
| INTESTINAL OBSTRUCTION | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
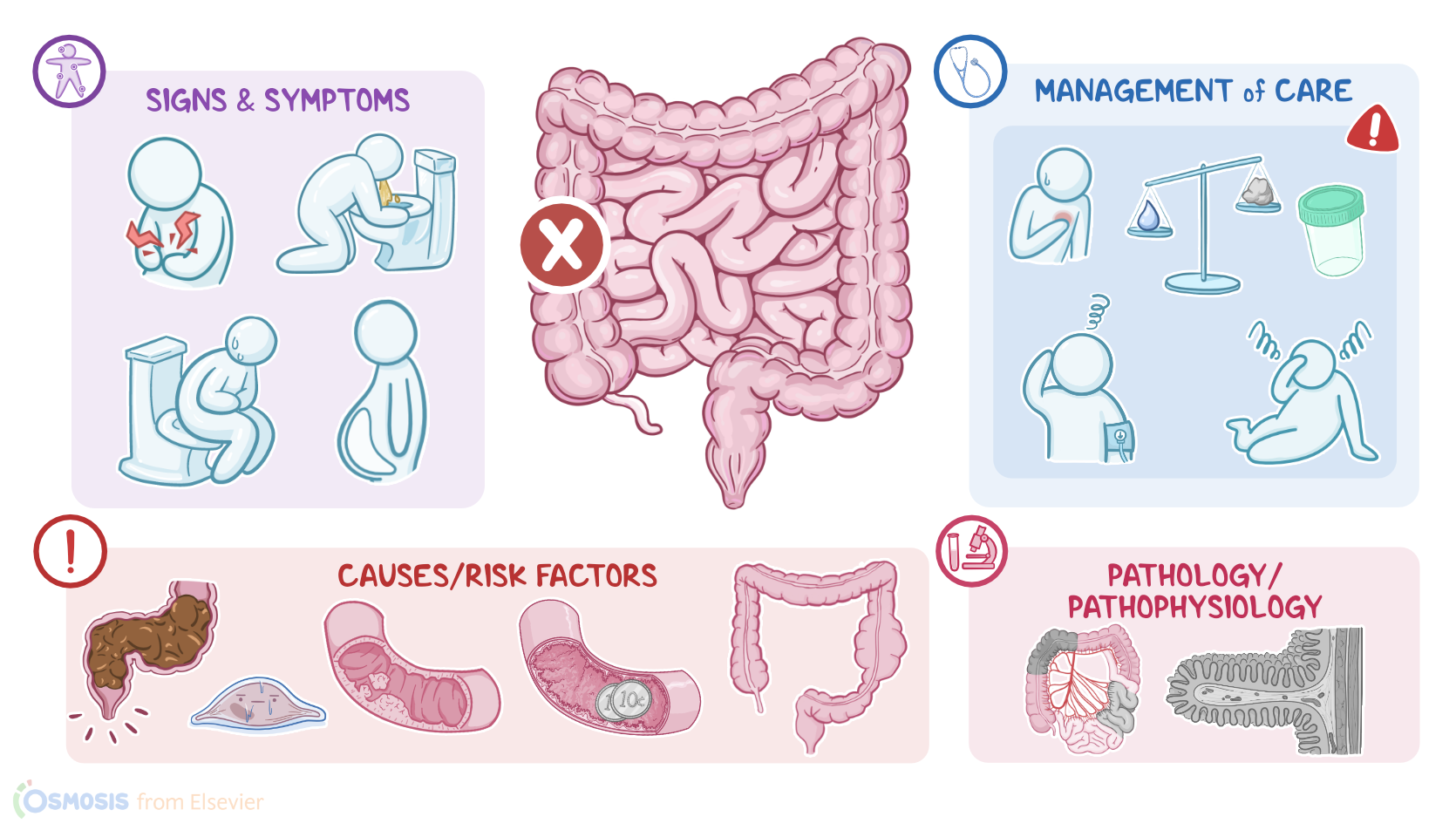
Intestinal obstruction is when the normal flow of contents moving through the small or large intestine is interrupted, causing problems with nutrient and fluid absorption and waste elimination.
Okay, first, let’s recall the physiology of the intestinal tract. The small and large intestines are tube-shaped structures through which the partially digested food, fluid and air pass through. After the intestines absorb the nutrients and fluid, the stool is formed and passed further until excreted.
Let’s zoom into the wall of the intestine, which is made up of four layers. The outermost layer is called serosa or adventitia, that faces the abdominal or peritoneal cavity. This is the space between the abdominal wall and abdominal organs that is lined with peritoneal membrane and contains a small amount of serous fluid. Next is the muscular layer, which contracts to move food through the bowel, and this is called peristalsis. After that is the submucosa, which consists of a dense layer of tissue that contains blood vessels, lymphatics, and nerves. And finally, there’s the innermost layer, called the mucosa, which contains the epithelial lining, facing the lumen, that enables nutrients and fluid absorption.
The causes of bowel obstruction can be either mechanical or functional; and the latter is also called ileus. Mechanical obstruction is caused by actual blockages in the small or large intestine, and it can be defined as partial or complete, as well as simple or strangulated. Partial obstruction is when gas or liquid stool can pass through the point of narrowing, while with complete obstruction, nothing is able to pass through. Now, there’s also simple mechanical obstruction, which is when the obstructed segment of the intestine maintains its blood supply, and strangulated mechanical obstruction, which is when blood supply has been compromised.
On the other hand, functional causes disrupt peristalsis, so even without a blockage, food, liquids and gas don’t move through the intestines.
Okay, so for the mechanical causes for intestinal obstruction, the most common one is postoperative adhesions, or bands of fibrous tissue that develop during the healing process following a surgical procedure. Other causes of mechanical obstruction include hernias, where a portion of the intestine protrudes out of the abdominal cavity and can get trapped or tightly pinched at the point where it pokes out; volvulus, which is when a loop of intestine twists upon itself, kinking off the lumen; and intussusception, which is where a part of the intestine folds into the lumen of an adjacent section of bowel, kind of like retracting a telescope.
Finally, mechanical obstruction of the intestine can be caused by strictures and fibrous bands, as well as tumors, fecal impaction, and ingestion of a foreign body, which can get lodged along the gastrointestinal tract.
Now, regarding functional obstruction, causes include anything that decreases smooth muscle contractility. The most common one is postoperative ileus, which is transient paralysis of the smooth muscles in the intestinal wall, and it’s usually caused by trauma during surgery. Other causes of functional obstruction include infections or inflammation, such as appendicitis, hypothyroidism, and intestinal ischemia, due to a thrombus or embolus. Finally, functional obstruction of the intestine can be caused by electrolyte abnormalities, such as hypokalemia and hypercalcemia, and various medications, including opioids.
Now, the risk of developing intestinal obstruction is higher in older clients, and those who have had abdominal or pelvic surgery. In addition, clients with inflammatory bowel disease, like Crohn's disease, endometriosis, and those who have had radiation therapy are also at an increased risk of developing strictures, which can lead to intestinal obstruction.
Okay, let’s go over the pathology of intestinal obstruction. So, regardless of the cause, when there's an intestinal obstruction, the bowel contents distal to the obstruction get passed; but after that happens, proximal to the obstruction, gas and stool start to accumulate, causing the bowel to dilate, and therefore, the overall abdominal cavity to distend. Over time, all this gas and stool increases the pressure inside the bowel lumen, so the intestinal contents push towards the intestinal wall, compressing the mucosal blood and lymphatic vessels. Since the walls of veins and lymphatics are weaker and easier to compress compared to arteries, venous and lymphatic drainage are the first ones to get blocked. The pressure pushes the water in these vessels into the surrounding tissue, leading to mucosal edema, inflammation, and damage. The overall result is the compromised ability of the mucosa to absorb nutrients and water, leading to fluid and electrolyte loss. If pressure inside the lumen gets even higher, it also compresses mucosal arteries, causing ischemia or reduced blood flow, which results in hypoxia of the intestinal wall.
Now, complications of intestinal obstruction include severe hypovolemia, as well as sodium, potassium, and chloride imbalance. This can lead to acute kidney injury and a life-threatening hypovolemic shock, where blood flow to the vital organs is compromised. At the same time, intestinal ischemia might extend from just the mucosa to all layers of the bowel wall, known as a transmural infarction or strangulation. This may result in bowel perforation, so there’s basically a hole in the bowel wall that connects the lumen to the peritoneal cavity. And all the bacteria from the bowel lumen can now easily leak out, causing bacterial peritonitis. Now, since the layers of the peritoneum are very rich in blood vessels, large numbers of bacteria from the peritoneal cavity can sneak into the bloodstream, triggering a massive inflammatory response called sepsis, which can progress to septic shock and even death.
Generally speaking, clinical manifestations of intestinal obstruction include cramping, abdominal pain, constipation, vomiting, and abdominal distention. Now, the presentation of these symptoms can vary depending on the affected segment of the intestines. So, in clients with proximal small bowel obstruction, symptoms typically include copious vomiting, which is usually projectile, and contains bile or undigested food, along with minimal abdominal distension. In clients with distal small bowel obstruction, vomiting is not that frequent, but when it occurs, it is typically foul-smelling and may contain feces; whereas abdominal distention is more pronounced compared to proximal small bowel obstruction. Finally, clients with large bowel obstruction typically present with late onset vomiting or no vomiting at all, and significant abdominal distension.
Sources
- "Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. 12th Edition. ISBN: 978-0-323-78961-5 " Elsevier (2023)
- "The Oncological Emergency of Intestinal Obstruction: ED recognition and Treatment Outcomes. 37(5):151207." Seminars in Oncology Nursing (2021)
- "Seidel’s guide to physical examination (10th ed). ISBN 9780323481953 " Elsevier (2023)
- "Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. 11th Edition. ISBN: 978-0-323-55149-6 " Mosby (2019)
- "Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care. 10th Edition. ISBN: 978-0-323-61242-5 " Elsevier (2020)
- "Prediction model for irreversible intestinal ischemia in strangulated bowel obstruction. 22(1), 321. " BMC surgery (2022)
- "Simultaneous occurrence of acute appendicitis and appendicular band syndrome in a patient with intestinal obstruction. 31:101637." Visual Journal of Emergency Medicine (2023)