Laryngotracheobronchitis (LTB) and croup: Nursing process (ADPIE)
Laryngotracheobronchitis (LTB) and croup: Nursing process (ADPIE)
Watch later
Watch later
Notes
| LARYNGOTRACHEOBRONCHITIS (LTB) AND CROUP | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Two year old Sara Little is brought to the Emergency Department, or ED, by her mother.
She has a high-pitched, barking cough that started in the evening and worsened throughout the night.
Mrs. Little explains that Sara has had “cold symptoms” for about 3 days.
She initially had a runny nose and slight cough but began running a fever yesterday.
She hasn’t been eating or drinking well and seems more anxious and difficult to soothe at night.
When Mrs. Little noticed wheezing, she called the pediatrician who directed her to bring Sara to the ED.
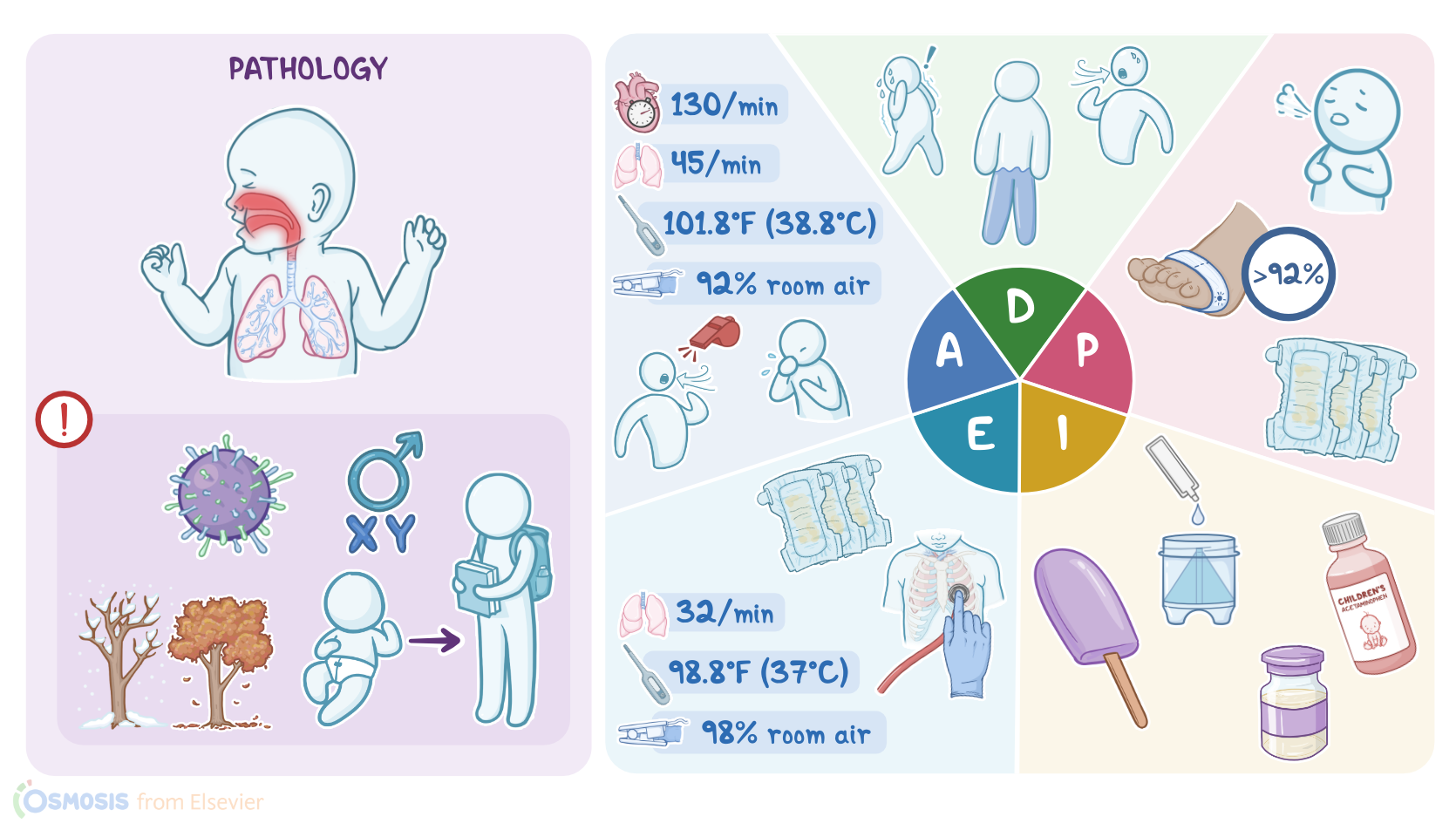
Upon arrival, Sara has a barking cough, inspiratory stridor, and a respiratory rate of 42 per minute.
Sara will be treated for laryngotracheobronchitis, or LTB, also known as croup.
Croup is an inflammation of the upper airway, typically caused by a virus, such as parainfluenza, adenovirus, influenza A or B, or respiratory syncytial virus, or RSV.
Cases of croup are seen seasonally, most often in late fall and early winter.
It affects children ages 3 months to 6 years and is most common in boys and in children where there is a family history of croup or recurrent croup.
Croup is spread through airborne respiratory droplets, saliva and physical contact with an infected person or contaminated surface.
The droplets enter the body, initially infecting the nasal passages and pharynx, subsequently spreading to the larynx, trachea and bronchi.
The infection causes inflammation, edema and mucus secretion, leading to narrowing of the subglottic area, which is composed of the lower part of the vocal cords and the upper trachea.
Not only is this area the narrowest portion of a child’s upper airway, but it has a complete ring of cartilage around it which doesn’t expand.
When the airway becomes significantly narrowed, it results in hoarseness, a harsh high-pitched sound during inspiration referred to as inspiratory stridor, and a distinctive seal-like barking cough.
Nasal flaring, substernal, subcostal or intercostal retractions occur as the child works hard to breathe past the narrowed airway.
Crying and agitation causes increased oxygen demand and further airway obstruction.
In addition, dehydration may result due to reluctance to drink fluids, fever, and breathing through the mouth.
Signs of severe croup include fatigue and inability to keep up with the needed respiratory effort resulting in diminished breath sounds, hypoxia, and cyanosis.
Eventually, inadequate ventilation can lead to respiratory acidosis and respiratory failure.
A diagnosis of croup is based on the client’s history and clinical findings.
Other diagnostic studies such as labs and radiological studies are not indicated unless there is concern for other serious problems such as pneumonia.
A chest X-ray, if done, will often reveal a pattern known as a steeple sign, which is an inverted V shape resembling a church steeple, visualized below the vocal cords.
Treatment of croup is focused on airway management and is guided by the severity of symptoms.
Commonly prescribed treatments include inhaled bronchodilators such as racemic epinephrine and albuterol; a corticosteroid like dexamethasone to decrease inflammation; and antipyretics such as acetaminophen to reduce fever.
Other treatments include humidified supplemental oxygen, and in the case of respiratory impending failure, intubation and mechanical ventilation.
OK, now that we understand croup, let’s get back to Sara and her mother.
You wash your hands and don a mask and gloves as you enter Sara’s room.
After introducing yourself and confirming Sara’s identity, you begin your assessment by asking Mrs. Little about how Sara has been feeling before coming to the ED.
Mrs. Little states Sara started to have a runny nose a few days ago and her fever started yesterday.
She hasn’t felt like eating or drinking and has had fewer wet diapers than normal.
The barking cough started this evening.
You gently approach Sara, keeping in mind agitation can further compromise her airway.
You can easily hear stridor with inspiration and the distinctive barking cough that characterizes croup.