Left-sided heart failure: Nursing process (ADPIE)
2,111views
Left-sided heart failure: Nursing process (ADPIE)
ER Nursing Week 2
ER Nursing Week 2
Notes
| LEFT-SIDED HEART FAILURE | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Jamal Hendrick is a 63-year-old male client who was admitted to the Medical-Surgical floor yesterday.
Mr. Hendrick has a history of chronic left-sided heart failure and hypertension.
He was directly admitted by his cardiologist after complaints of shortness of breath, dry cough, and severe fatigue.
He states his last hospitalization was around 6 months ago for similar symptoms.
Heart failure, also called congestive heart failure, is when the heart is unable to pump effectively enough to maintain cardiac output to meet the demands of the body.
Common risk factors for heart failure include uncontrolled hypertension, ischemic heart disease, valvular heart disease, cardiomyopathy, endocarditis, and acute myocardial infarction.
The onset of heart failure can be acute, which occurs suddenly and resolves in a short period of time, but usually develops slowly over a long period of time and persists as a chronic disease.
Often an individual can live with chronic heart failure, but then suddenly develop an acute exacerbation.
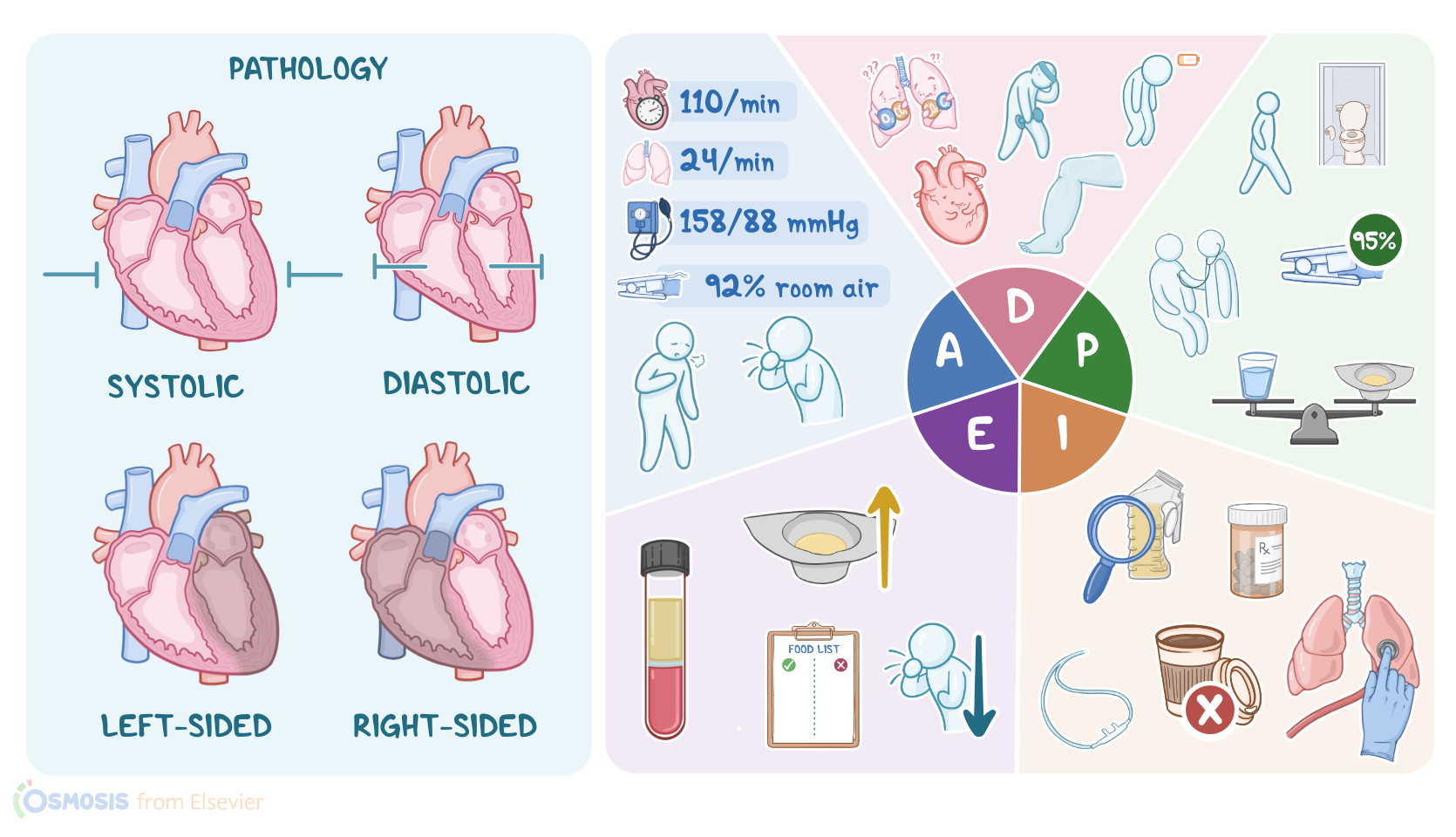
Heart failure can be the result of either systolic dysfunction, which is due to inadequate contractility, or diastolic dysfunction, when the heart is unable to relax and fill with blood.
Heart failure can affect the right side, the left side, or both sides of the heart.
The left and right sides of the heart are two separate pumping systems, and one side can remain functional for some time even if the other side is failing.
Most cases of heart failure initially start on the left side, and then eventually progress to include both sides.
With left-sided heart failure, the left ventricle is unable to pump with enough force to push blood into the aorta and the rest of the body.
When this happens, the blood remaining in the left side of the heart will back up into the lungs, causing pulmonary problems such as dyspnea, tachypnea, crackles, dry cough, paroxysmal nocturnal dyspnea, pulmonary edema, and pulmonary hypertension.
Pulmonary edema is a life-threatening emergency where the lungs fill up with fluid causing very high pressure.
Someone with pulmonary edema will present with a large amount of blood-tinged frothy sputum, severe dyspnea, tachycardia, profuse sweating, and cyanosis.
With right-sided heart failure, the right ventricle is not able to move blood forward into the lungs, causing it to back up into the superior and inferior vena cavae and the rest of the venous system.
Right-sided heart failure is almost always caused by left-sided heart failure, because increased pulmonary pressure from blood backing up into the lungs from the left side makes it more difficult for the right side to pump blood into the lungs.
As the right side works harder to overcome the increased pressure it eventually wears out and fails.
Symptoms of right heart failure include dependent edema, jugular venous distension, abdominal distension, splenomegaly, anorexia, weight gain, nocturnal diuresis, and hypertension or hypotension.
Certain mechanisms kick in to try to compensate for the decreased cardiac output.
Through the Frank-Starling mechanism, myocardial contractility is increased, which helps push blood forward.
The sympathetic nervous system also responds by increasing heart rate, increasing peripheral vascular resistance, and further enhancing cardiac contractility.
Sodium and water is retained through the actions of the renin-angiotensin-aldosterone system, which provides additional circulating volume.
The ventricular cells, or myocytes, undergo remodeling, resulting in changes such as increased muscle mass and thickening of the ventricular wall.
These compensatory efforts will initially lead to an increase in cardiac output, but over time the heart will be overburdened and less efficient.
When this happens, clinical symptoms of heart failure will appear. Without treatment, heart failure will progress and result in complications such as pleural effusion, cardiac dysrhythmias, and renal failure.
Okay, let’s get back to our client.
Upon entering Mr. Hendrick’s room, you introduce yourself, confirm his identity, and wash your hands.
You begin your assessment of Mr. Hendrick by asking him how he is feeling today.
He tells you he feels short of breath, but better than when he was admitted.
Mr. Hendrick goes on to say he is extremely tired today, and that he has been feeling fatigued for several days.
You ask Mr. Hendrick what caused him to start feeling short of breath, and he replies he just walked to the bathroom.
You notice he pauses several times during your chat to cough, but it’s non-productive.
You ask Mr. Hendrick if he has issues breathing at night, he replies he wakes up every night with difficulty breathing and that he sleeps better in his recliner.
You ask Mr. Hendrick if he has been using the bathroom regularly, he states he has been urinating less than normal.
You check the bedside portable urinal and document 30 milliliters of clear yellow urine.
Upon visual inspection of Mr. Hendrick, you notice that in addition to appearing slightly short of breath, nasal flaring is present, he’s using his accessory muscles to breathe, and he’s diaphoretic.
You auscultate his lungs and hear wheezing on inhalation and crackles throughout both lobes.
You assess capillary refill and note that it is decreased.
Skin color and turgor are normal.
Mr. Hendrick’s vital signs are HR: 110, RR: 24, BP: 158/88, oxygen saturation: 92% on room air, oral temp.: 98.2° F, pain: 0/10.