Meconium aspiration syndrome: Nursing
Meconium aspiration syndrome: Nursing
Acute Final
Acute Final
Notes
| MECONIUM ASPIRATION SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
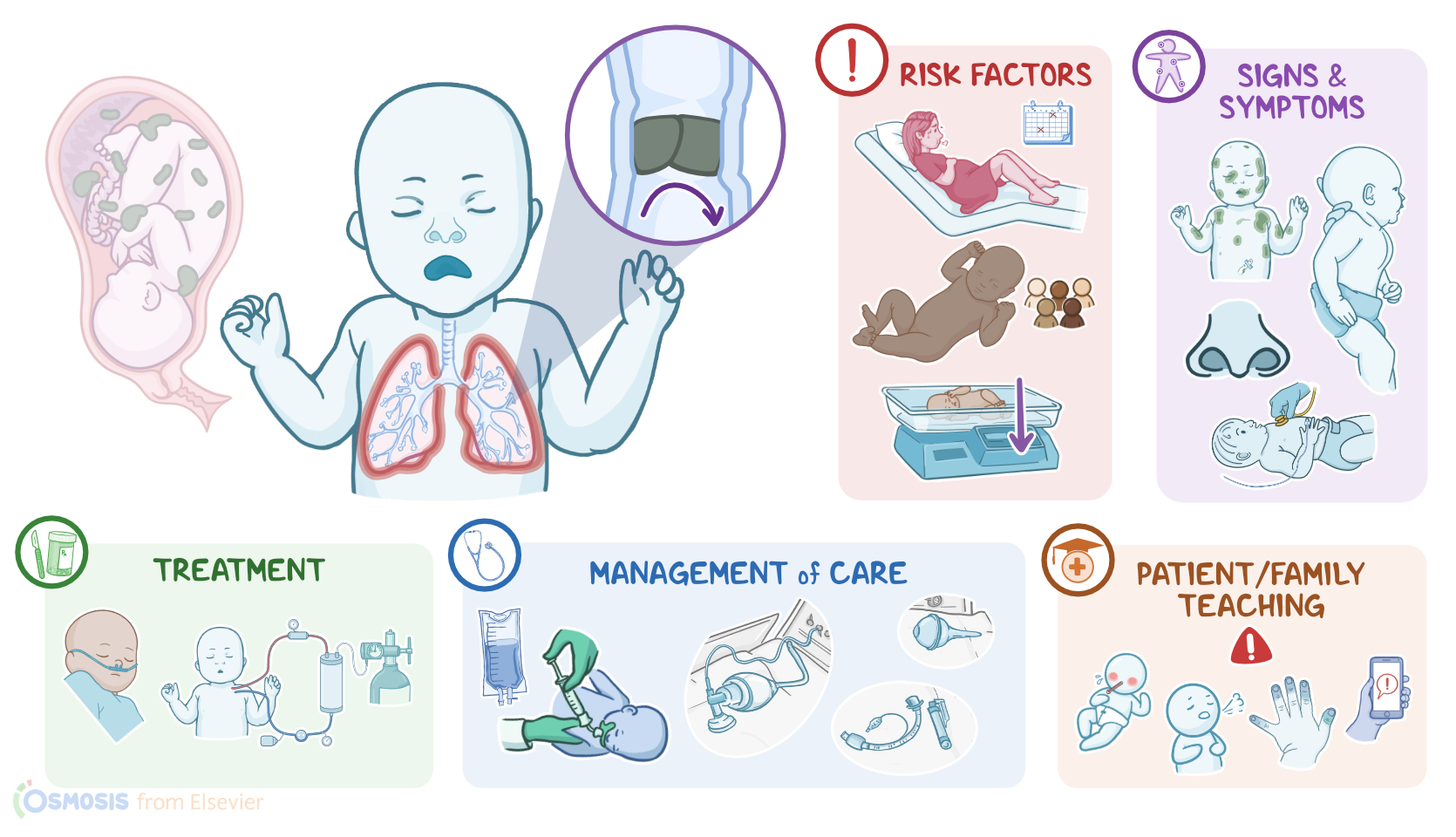
Meconium aspiration syndrome, or MAS for short, is a condition characterized by respiratory obstruction and distress caused by meconium entering the respiratory tract. Now, meconium is a thick, sticky, green-black substance that is the first stool of the newborn. It starts forming as early as the 12th week of gestation, and it’s made up of amniotic fluid, mucus, cells that have been shed from the skin or intestinal tract, and intestinal secretions, like bile. Normally, the meconium is passed by the newborn within the first 48 hours of life. All right, now the exact cause of meconium aspiration syndrome is unknown, but it’s believed to be initiated by a stressful intrauterine event that leads to the early passage of meconium. Risk factors for developing meconium aspiration syndrome include anything that can cause stress to the fetus, such as hypoxia, or low levels of oxygen in the fetal blood, caused by problems like compression of the umbilical cord, insufficiency of the placenta, or prolonged labor.
Meconium aspiration syndrome is also more common among post term infants, especially if they are small for gestational age. Other risk factors include babies who are Black or South Asian, as well as Pacific Islanders and indigenous Australians. The pathology of meconium aspiration syndrome starts with an intrauterine stressful event that leads to inadequate oxygen delivery to the fetus and subsequent hypoxia. Hypoxia causes increased intestinal motility and relaxation of the anal sphincter, which stimulates meconium excretion into the amniotic fluid, as well as fetal gasping, which can allow meconium to be aspirated into the respiratory tract. Meconium can also be aspirated spontaneously or when the baby takes the first breath after delivery. Now, aspiration of meconium can cause a number of complications. First, the bile salts and pancreatic enzymes contained in the meconium cause chemical pneumonitis.
In addition, meconium occludes the airways with a ball-valve mechanism that allows air in but obstructs airflow out during expiration. This leads to air trapping, alveolar collapse, and possible pneumothorax.Other complications include inhibition of surfactant production, and pulmonary vasoconstriction, which can progress to persistent pulmonary hypertension. Clinical manifestations of meconium aspiration syndrome include signs of respiratory distress including shallow, rapid breathing, along with grunting, nasal flaring, and chest retractions. In severe cases, the infant may also appear cyanotic. There is often a barrel-shaped chest, due to the air trapping in the lungs. During auscultation, abnormal breath sounds can also sometimes be heard, such as crackles, rales, or rhonchi. Other signs include staining of the nails, skin, and umbilical cord with meconium.
The diagnosis of meconium aspiration syndrome starts with the perinatal history and physical assessment, followed by a chest X-ray, which may show patchy infiltrates of the lung, lung consolidation, and hyperexpansion due to air trapping. Arterial blood gas or ABG analysis may show hypoxemia, hypercapnia, and respiratory acidosis. After delivery, the treatment of meconium aspiration syndrome depends on the status of the newborn. So, a vigorous infant with a heart rate of over 100 beats per minute, spontaneous respirations, and good muscle tone will need routine care and close monitoring. On the other hand, infants making poor attempts to take their first breath or have otherwise depressed respirations, current options include continuing with resuscitation measures and transferring to the neonatal intensive care unit, or NICU. Further treatments may include antibiotics to prevent infections, ventilatory support, chest physiotherapy to loosen secretions, and surfactant administration to replace endogenous surfactant.
Lastly, if persistent pulmonary hypertension develops, inhaled nitric oxide or extracorporeal membrane oxygenation might be necessary. Okay, let’s look at the nursing care you’ll be providing for a client with meconium aspiration syndrome. Priorities of nursing care are to provide effective resuscitation and supportive care. After delivery, work with the healthcare team to provide neonatal resuscitation measures, including placing the baby on a radiant warmer, drying and removing the wet linen, and gently stimulating the baby. Then, position the baby in a sniffing position and suction with a bulb syringe, if needed. Assist with additional interventions as indicated, including administration of oxygen, positive pressure ventilation with bag-valve mask, or intubation; and transfer the baby to the neonatal intensive care unit, as indicated.