Paget disease of bone: Nursing
Paget disease of bone: Nursing
T & P 3 Altered Musculoskeletal
T & P 3 Altered Musculoskeletal
Notes
| PAGET DISEASE OF BONE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Contributors
Paget disease of bone is a disorder in which there’s a lot of bone remodeling that happens in some regions of the bone. Typically, there’s excessive bone resorption followed by disorganized and excessive bone growth, leading to skeletal deformities, fragile bones, and potential fractures. Paget disease of bone can affect a single bone or several bones, and most often, it involves the skull, spine, pelvis, arms, and legs.
Now, let’s quickly review the physiology of bones.Normally, the surface of the bones is covered by a dense layer of connective tissue called the periosteum, and it's where the muscles, tendons, and ligaments are attached.
Beneath the periosteum, there’s a dense and tough external layer called compact bone or cortical bone composed of collagen and hydroxyapatite which contains calcium and phosphate.
In the center of the bone, there’s the medullary canal, a hollow space lined by a honeycomb- looking structure called the spongy or cancellous bone. The spaces in the spongy bone are occupied by the bone marrow, which is the site of blood cell production.
At first glance, a bone may appear inert and unchanging, but it’s actually a very dynamic tissue. In general, a bone is replaced with new cells every three to ten years in a process called bone remodeling, which has two steps: bone resorption, when specialized cells called osteoclasts break down bone, and bone formation, which is when another type of cells called osteoblasts form new bone.
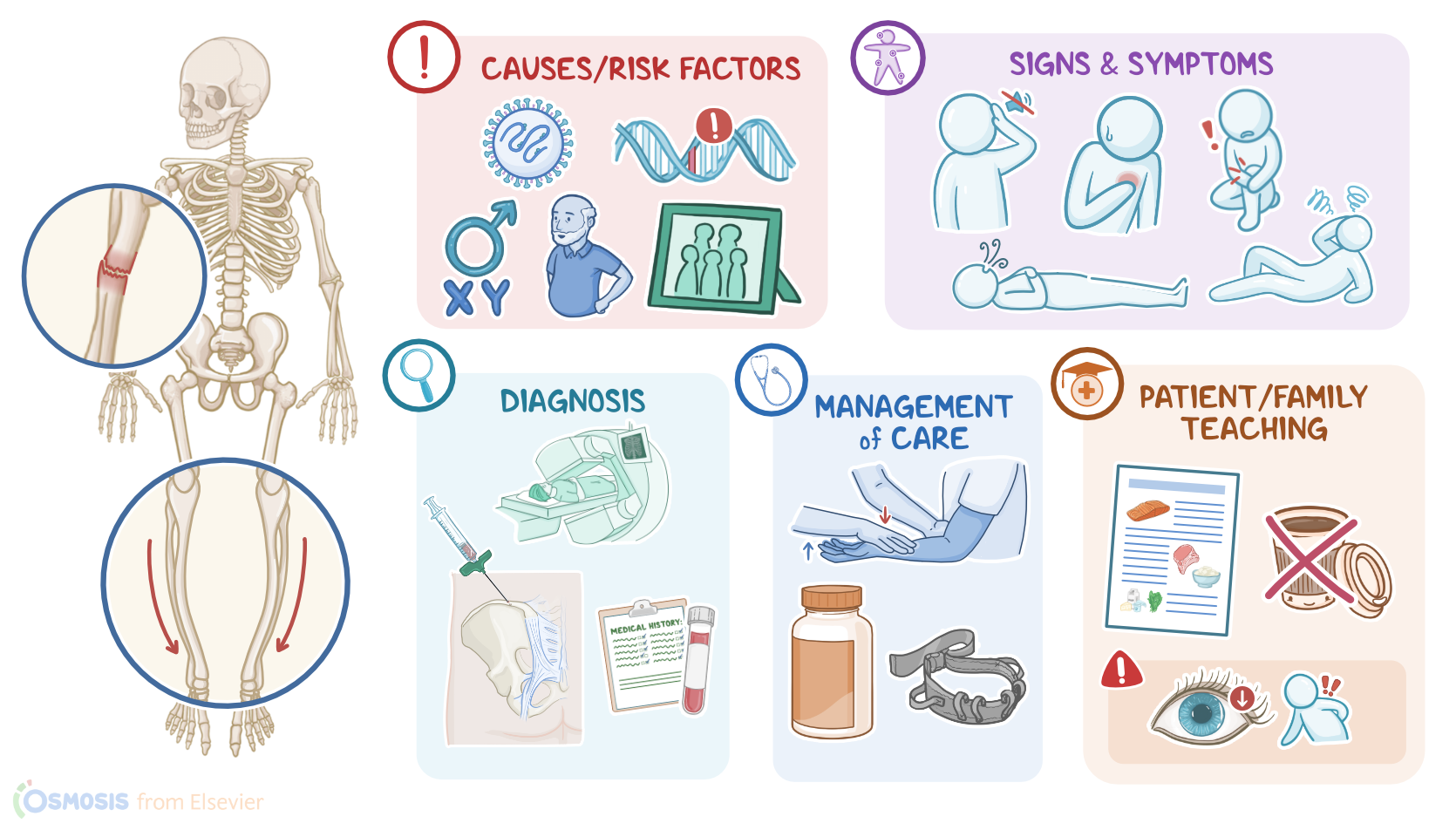
The exact cause of Paget disease of bone is unclear, with some theories suggesting that it can get triggered by infections like the measles virus, and is linked to genetic mutations. Risk factors include being assigned male at birth, age over 40, family history of Paget disease, Caucasian race, or northern European descent.
The pathology of Paget disease has three phases, called lytic, mixed, and sclerotic phases. Phase one is the lytic phase, and that’s where osteoclasts increase in number and activity to aggressively demineralize the bone.
Phase two is the mixed phase where the lytic phase continues but the blastic phase also starts. In the blastic phase, there’s a rapid but disorganized proliferation of new bone tissue by an increased number of osteoblasts. The result is that collagen fibers are deposited in a haphazard way.
Phase three is the sclerotic phase, and that’s where new bone formation exceeds bone resorption, and the net result is more bony matter, but the bones are structurally disorganized and therefore weaker than healthy bones. At the same time, osteoclasts secrete molecules that induce new blood vessel formation, resulting in an increased vascularization of the sclerotic bone. Eventually, the osteoblastic activity also slows down, and there’s a dormant state in the disease, called the “burned-out state.” Finally, in rare cases, the accelerated bony growth can lead to genetic mutations that cause a type of bone cancer called osteosarcoma. When that happens it’s referred to as Paget sarcoma.
Clinically, clients with Paget disease often have no symptoms. But when symptoms are present, they can experience fragility fractures, where the bones are so weak that they break with minimal force, like bumping into a door, or even spontaneously from the weight of the body alone.
Over time, clients can also develop bone pain that ranges from mild to severe, as well as bone deformities, such as bowing of the legs.
Paget disease of bone can also cause neurological symptoms. Misshapen and overgrown bones in the vertebral column can impinge on the spinal nerve roots.
In severe cases, there can also be compression of the cauda equina, which is the bundle of nerves protruding from the bottom of the spinal cord that resembles a horse's tail.
This is a rare but dangerous condition where the client will experience severe lower back and leg pain, weakness and sensation loss in the lower extremities, especially the “saddle region” which includes the inner thigh, groin and buttocks and loss of bladder and bowel control.
Bone overgrowth can also narrow the auditory foramen or optic canal and impinge on the auditory nerve or optic nerve respectively. This can cause hearing or vision loss, respectively.
Next, if the parts of the bone that are involved in a joint are involved, it can result in osteoarthritis. This can cause joint pain and stiffness. If the skull is involved, the overgrowth of bones can cause headache. It could also change the shape of the client’s face which is sometimes described as a “ lion- like” appearance and this is called leontiasis.
In addition, increased vascularization of the new bone means that the heart has to work harder to keep up with the increased blood supply. In severe cases, this can progress to heart failure, which can cause manifestations like orthopnea.
Another cardiovascular complication of Paget disease of bone is calcification of the aortic valve, which can lead to aortic stenosis and cause manifestations like dyspnea, particularly during exercise; fatigue; and syncope.
The diagnosis of Paget disease of bone starts with the client's history and physical assessment, followed by blood tests, which typically reveal elevated levels of alkaline phosphatase, which gets released into the blood as bone is destroyed, with normal calcium and phosphate levels.
Urinalysis can show increased markers of collagen degradation, especially during the lytic and mixed phases.
In addition, an X-ray might show lytic lesions during the lytic phase of the disease, and sclerotic lesions which are thickened and dense areas that develop over time.
A CT or MRI scan, as well as a bone scintigraphy can also be done to identify lesions.
Finally, a bone biopsy is usually done to exclude malignancies which can mimic some of the findings of Paget disease of bone.
Now, the treatment of mild forms of Paget disease of bone can rely on monitoring the client’s condition, if they are asymptomatic and don’t have any significant laboratory or imaging changes . Otherwise, treatment is focused mainly on pain management, with NSAIDs or acetaminophen, and trying to limit bone resorption with bisphosphonates like zoledronic acid, risedronate or alendronate. For clients who can’t tolerate bisphosphonates, subcutaneous injections of calcitonin can be given.
Calcium and vitamin D prescriptions are sometimes also administered to correct hypercalcemia before starting treatment with bisphosphonates.
Finally, surgery can help correct bone deformities, decompress an impinged nerve, and reduce associated fractures.