Postoperative care: Nursing
1,821views
Notes
| POSTOPERATIVE CARE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Postoperative care is the management of a client’s health during the postoperative period. This begins right after the surgical procedure is complete, and lasts until the client is discharged from the healthcare facility. Postoperative care promotes the client’s recovery after surgery by managing pain, supporting oxygenation and cardiovascular stability, maintaining fluid balance, providing wound care, monitoring bowel function, assisting with mobility, and preventing complications.
Postoperative care typically begins when the client is transferred from the operating suite to the postanesthesia care unit, or PACU for short. How long they’re being cared for in this setting depends on the client’s health status, the type of procedure, and the type of anesthesia, as well as the rate of progression to alertness and hemodynamic stability. The goal of this phase of care is to stabilize the client for transfer to the next level of care, which could be an intensive care unit or another inpatient care unit; as well as being discharged home in the case of ambulatory surgery. In order for clients to transition to a different level of care, they should meet certain criteria such as responding easily to stimuli, having stable vital signs, and adequate pain control.
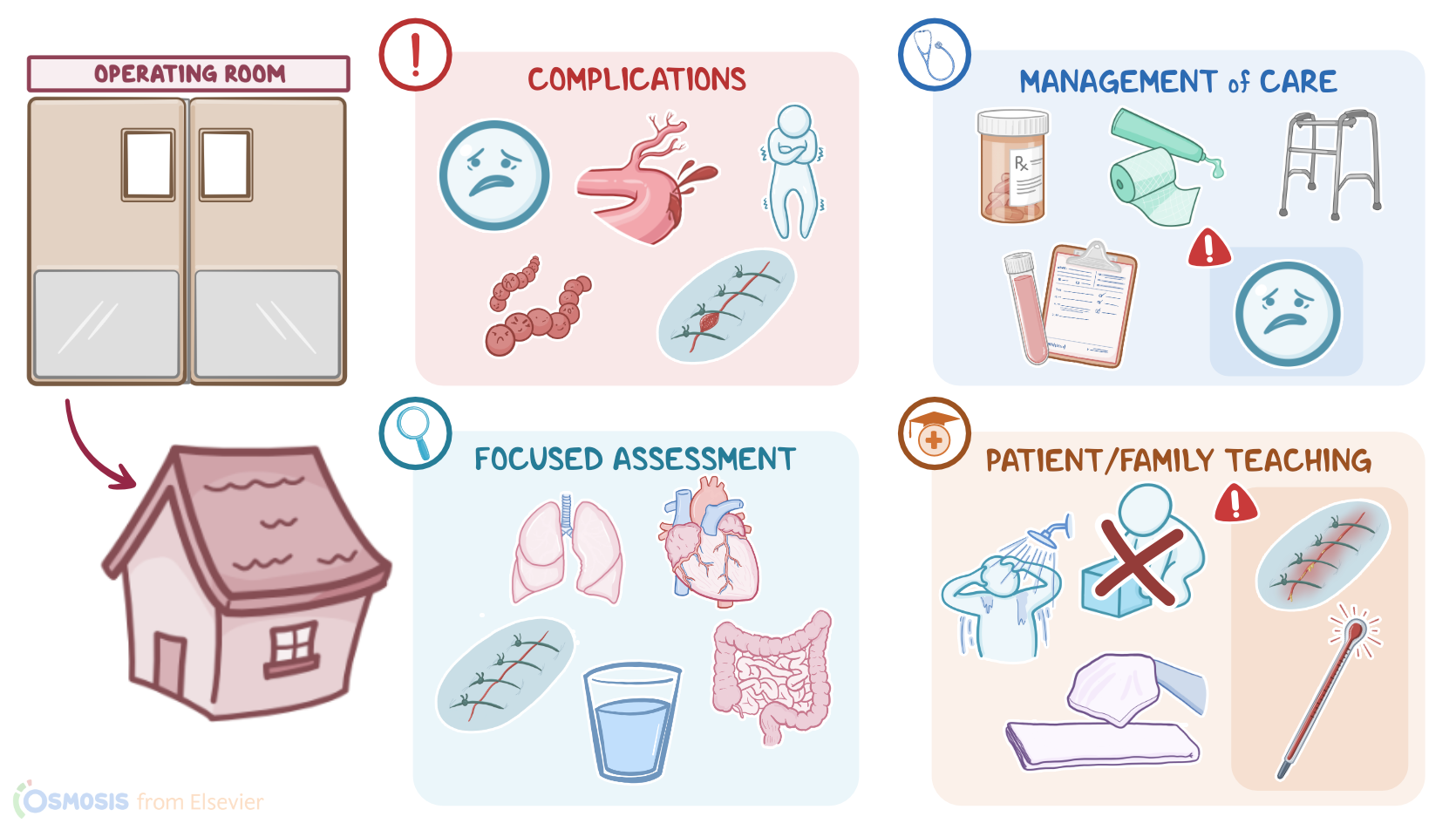
Now, the most common complications during the postoperative period include pain, hemorrhage, hypothermia, and infections at the site of the surgery, called surgical site infection, or SSI for short, as well as wound dehiscence and evisceration. There can also be respiratory complications, like airway obstruction, laryngospasm, pneumonia, atelectasis, and pulmonary embolism.
Cardiovascular complications can also occur, such as hypotension, hypertension, and dysrhythmias. Clients can also develop nervous system complications, including delirium and delayed emergence from anesthesia.
On the other hand, gastrointestinal complications include postoperative nausea and vomiting, constipation, postoperative ileus, and hiccups; while urinary complications can manifest as urinary retention and urinary tract infections. Finally, fluid and electrolyte imbalances can also occur following surgical procedures.
Okay, let’s look at the care you’ll provide to a client during the postoperative period. Your priority goals of care are to facilitate a smooth transition of care from the PACU, monitor for postoperative complications, and provide supportive care.
Now, when your client is transferred out of the PACU to your clinical unit, obtain a complete handoff report from the PACU nurse, including the client’s name; age; the names of the surgeon and anesthesia care providers; the procedure performed and type of anesthesia used; as well as airway status, pain management; NPO status; and orders that need to be implemented.
Ask about the intraoperative course, including medications administered; length of time the client was under anesthesia and reversal agents used; estimated blood loss and total volume of fluids replaced; any unexpected events and how they were managed; and results of diagnostic tests.
Then, along with the PACU nurse, check the incisional site and dressing, and locate any drains, tubes, or catheters that were placed during surgery. Also check the IV site, solutions, and infusion rate. Lastly, be sure to collect information about the client’s medical history, medications, allergies, the use of assistive devices such as glasses, hearing aids, or walkers, as well as their primary language, emotional status, available social support, and cultural or spiritual preferences.
Begin a focused assessment, starting with their respiratory status. Check their airway patency, and adequacy of gas exchange. Encourage them to take deep breaths, and show them how to splint their incision while coughing. Remind them to use their incentive spirometer, and assist them to change position regularly to promote perfusion to both of their lungs.
Report to the health care provider if your client has signs of airway obstruction such as inspiratory stridor; signs of atelectasis like decreased breath sounds or a SpO2 less than 95%; or other indications of respiratory compromise such as tachypnea, dyspnea, or chest wall retractions. As prescribed, administer supplemental oxygen, reposition them to allow for full chest expansion, and monitor their response to treatment.
Next, assess your client’s cardiovascular status. Report to the healthcare provider if there’s a systolic blood pressure less than 90 mmHg or greater than 160 mmHg; a heart rate is less than 60 beats per minute or greater than 120 beats per minute; a narrow pulse pressure; or any changes to the heart rhythm. Administer corrective medications as prescribed and implement advanced cardiovascular life support measures if needed.
Additionally, report to the healthcare provider any signs of hemorrhage or shock, such as a weak, rapid, thready pulse; hypotension; or cool, clammy skin. Apply pressure to sites of active external bleeding; administer supplemental oxygen; increase the IV flow rate; and administer blood products as prescribed. Elevate their legs unless contraindicated; and prepare your client for surgery if indicated.
Also assess your client’s peripheral vascular status. Apply antiembolism stockings or sequential compression devices; plan early ambulation to promote venous return; and administer prophylactic anticoagulants as prescribed. Report to the healthcare provider if signs of a venous thromboembolism develop, including leg pain with warm skin tender to the touch; or signs of a pulmonary embolism, such as sudden dyspnea, sharp chest pain, tachycardia, and cyanosis. Administer supplemental oxygen and prepare your client for further intervention.
Okay, now, you’ll also need to complete a neurologic assessment by checking their level of consciousness, orientation, and ability to follow simple commands. Check sensation and ability to voluntarily move their extremities. Report to the healthcare provider if your client has an alteration in mental status, provide reassurance, and work with the interdisciplinary team to identify and treat the underlying cause.
Be sure to keep a close eye on your client’s incision site, dressings, and surgical drains. Perform dressing changes, wound care, and maintain patency and suction of surgical drains.