Postpartum hemorrhage: Nursing
1,735views
Postpartum hemorrhage: Nursing
Acute Final
Acute Final
Notes
| POSTPARTUM HEMORRHAGE (PPH) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Postpartum hemorrhage or PPH is an obstetrical emergency which occurs when there is any significant loss of blood after delivery of a baby. Now, some blood loss is expected during childbirth, but PPH is when the blood loss during the first 24 hours exceeds 500 mL after vaginal birth or 1000 mL after cesarean delivery. Significant bleeding in the first 24 hours after delivery is called early or primary postpartum hemorrhage, while late or secondary postpartum hemorrhage occurs 6 weeks to 12 weeks after birth.
Okay, let’s start with some physiology. So, after delivery, the uterus tends to regress back to its normal size and resume its pre-pregnancy position by the sixth week, a process known as involution. Immediately after the delivery of placenta, the smooth muscles of the uterus continue to contract and squeeze down on the placental arteries where they are attached to the uterine wall, causing them to clamp them shut and reduce uterine bleeding.
There are also some physiological changes that occur during pregnancy that begin to change back to pre-pregnancy levels in the postpartum period. For example, during pregnancy there is increased blood plasma volume in relation to red blood cell mass. As a consequence, maternal hemoglobin and hematocrit are usually relatively low during pregnancy, since the same amount of red blood cells are circulating in a higher volume of blood. After delivery, through increased diuresis or urine production, and increased diaphoresis or sweat production, blood volume returns to normal in about 6 to 12 weeks, and hemoglobin, and hematocrit levels normalize in 4 to 6 weeks. Likewise, during pregnancy, plasma fibrinogen and other pro-coagulant factors increase, and they stay elevated until 4 to 6 weeks following delivery.
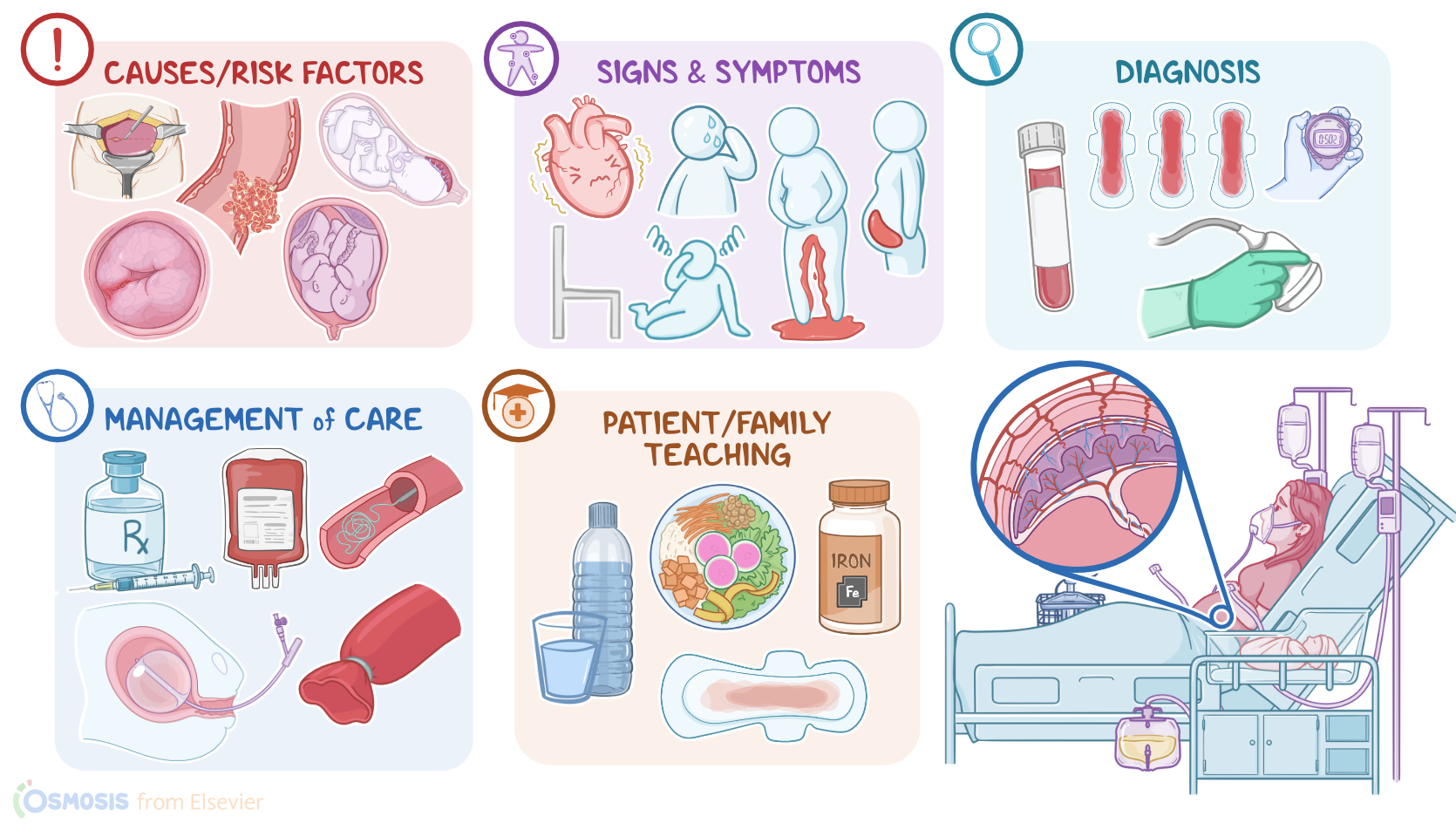
The most common causes of postpartum hemorrhage can be divided into two groups; the early causes and the late causes. The early causes can easily be remembered as the 4 Ts: Tone, Trauma, Tissue, and Thrombin.
Tone refers to a lack of uterine tone, meaning the uterine contraction is weak or absent. This is also known as uterine atony, which is the most common cause of PPH. Repeated distention of the uterus as a result of multiple previous pregnancies or overstretching from multigestational pregnancy can interfere with effective uterine contractions after birth and lead to uterine atony after birth. Uterine atony can also occur when uterine muscles become fatigued after prolonged labor, or if urine retention causes a distended bladder that interferes with uterine involution.
The next T is Trauma, and it refers to damage to any of the reproductive structures, like the uterus, cervix, vagina, or perineum during delivery.
Next is Tissue, which refers to when a part of the placenta is retained in the uterus after birth, interfering with the involution process.
Lastly, Thrombin, refers to the mother having some condition that prevents blood clots from forming normally, for example, a coagulation disorder like von Willebrand disease. These conditions can turn even a tiny bleed into a serious bleed due to the inability to form blood clots.
Finally, some risk factors for PPH which include a history of PPH in previous pregnancies; placental disorders like placenta previa, placenta accreta or placental abruption; an overdistended uterus due to polyhydramnios, multiple gestation, or macrosomic infant; infection, prolonged labor, and lastly delivery by cesarean section.
Clinically, postpartum hemorrhage can be overt, in which a large amount of blood loss can be assessed; or occult, which is when blood pools up somewhere inside the body or inside a hematoma. This can be within the uterus or in the pelvic or abdominal cavity. The lochia rubra, which is the vaginal discharge after delivery, can appear abnormal with large amounts of fresh blood and numerous large blood clots. Severe bleeding can cause signs and symptoms of hypovolemic shock, such as orthostatic hypotension, dizziness, tachycardia, palpitation, shortness of breath, and cold, clammy skin. Some clients can have a severe backache with a feeling of pelvic heaviness due to hematoma formation.
Abdominal inspection may reveal the uterine fundus to be above the expected level, which could indicate internal bleeding and formation of hematoma. With uterine atony, palpation can reveal a boggy, soft and enlarged uterus instead of a firm, contracted one. Vaginal examination can reveal bright red discharge with numerous blood clots, indicating that the uterus is the source of the bleed, and not a cervical or vaginal laceration. Finally, close inspection of the placenta after delivery can show some of the placenta has been left behind.