Postpartum infections: Nursing
Postpartum infections: Nursing
Watch later
Watch later
Notes
| POSTPARTUM INFECTIONS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
Transcript
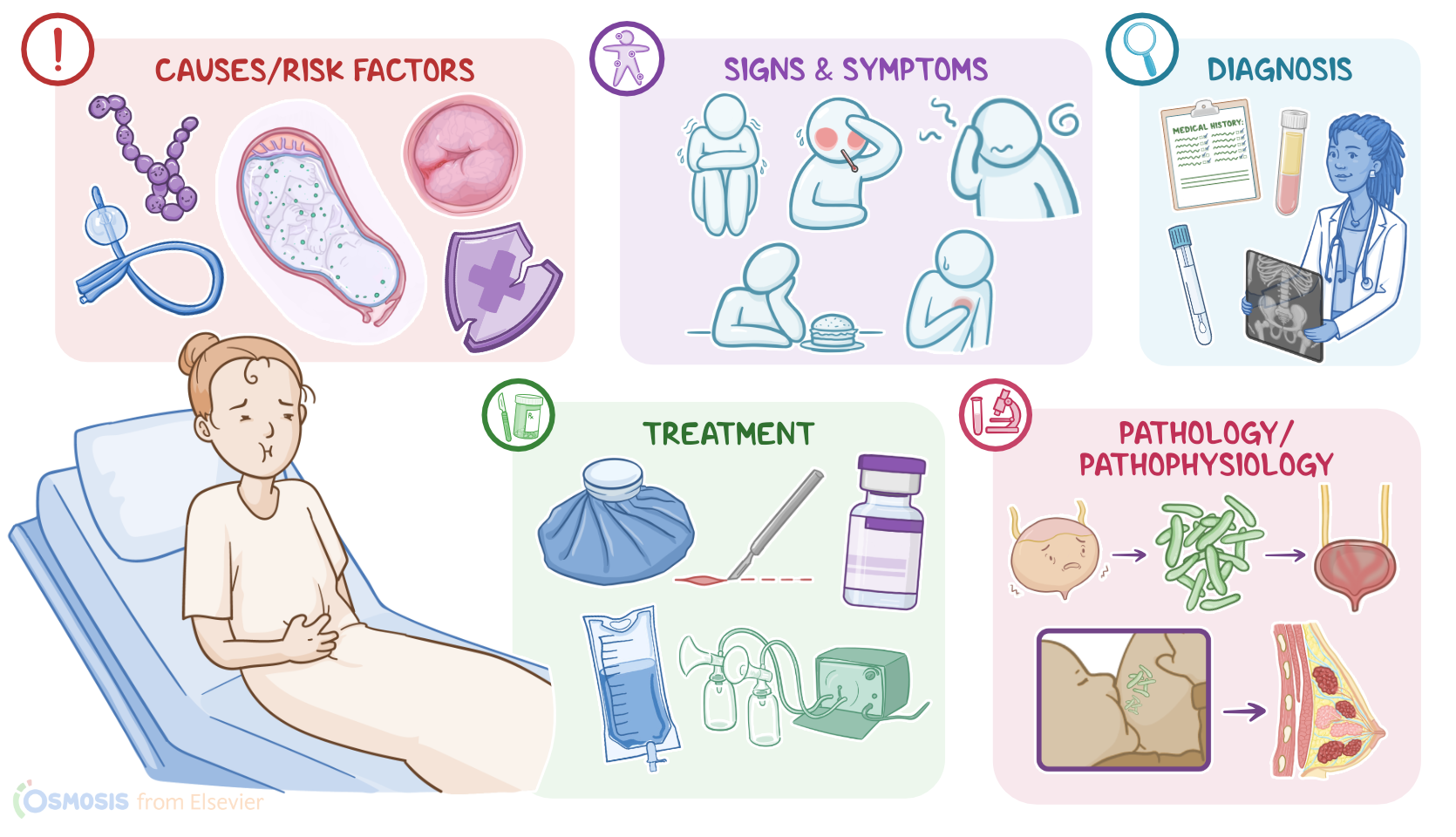
Postpartum, or puerperal infections are infections of the genitourinary tract, surgical wounds, urinary tract, and breast that develop after the first 24 hours and on any two of the first 10 days postpartum. First, let’s go over the physiology of the female reproductive system, which consists of the vulva, vagina, cervix, uterus, fallopian tubes and ovaries. The uterus is a hollow, pear-shaped organ that has an inner layer called endometrium and muscular layer called myometrium. During conception, the reproductive system undergoes changes that help support the fetus until birth, such as increased blood flow to the reproductive organs, increased uterine volume, weight, and fundal height, and increased activity of cervical mucus glands. After giving birth the uterus tends to regress back to its normal, pre-conception size and resume its pre-birth position, a process known as involution.
The thick superficial layer of the endometrium also sloughs off, and there is a discharge of lochia from the endometrium, cervix, and vagina. Okay, so postpartum infections are typically caused by aerobic or anaerobic bacteria, such as Eschericia coli, Proteus spp, Enterobacter spp, Klebsiella spp, Clostridium spp, Staphylococcus aureus, and Streptococci spp. Other less frequent pathogens include Chlamydia trachomatis, Ureaplasma, Mycoplasma, and Gardnerella vaginalis. Risk factors for postpartum infections of the genitourinary tract include colonization of the vagina with group A and B Streptococcus, chorioamnionitis, prolonged rupture of membranes, prolonged labor, as well as retained placenta tissue. In addition, internal fetal monitoring, like fetal scalp electrodes or intrauterine pressure catheters, and repeated vaginal examinations, seem to also increase the risk for postpartum infections.
Another important risk factor is trauma, which may involve abdominal wall trauma, as well as perineal tears, or lacerations to the endometrium, cervix, or vaginal mucosa. These may occur during normal childbirth, also known as physiological trauma, or while providing medical care, which is referred to as iatrogenic trauma. Examples of iatrogenic trauma include surgical wounds from cesarean delivery, and episiotomies, which are incisions made along the perineum to assist delivery. Next are risk factors for developing a postpartum urinary tract infection, which include the placement of a urinary catheter and urinary retention. Risk factors for developing postpartum mastitis include milk stasis, which can be caused by blocked milk ducts or inadequate breast emptying. Finally, clients who are immunocompromised, including those with HIV infection, cancer, malnutrition, diabetes, or those taking immunosuppressant medications like corticosteroids are at higher risk for all types of postpartum infections.
Okay, the pathology of a postpartum infection of the genitourinary tract often starts as an ascending infection, meaning bacteria start by colonizing the vagina, and then make their way up the cervix and uterus. Once the bacteria reach the uterus, they can infect the endometrium and myometrium, causing endometritis. In other cases, there’s trauma to the abdominal wall or perineum, which allows bacteria from the skin, vagina, or bowel flora to penetrate deeper into the subcutaneous tissue, abdominal and pelvic cavities. At the same time, after delivery, there’s commonly urinary retention in the bladder, which gives bacteria time to multiply and cause cystitis. In addition, mastitis can develop while breastfeeding. That’s because trauma to the nipple and areola, such as small skin cracks, enables bacteria from the skin or a newborn's mouth and nose to penetrate the breast itself.
Okay, in terms of complications, in the case of postpartum endometritis, bacteria can make their way to the fallopian tubes, causing salpingitis, the ovaries, causing oophoritis, or the peritoneum, causing peritonitis. Bacteria can also invade the pelvic venous system causing inflammation and damage of the venous wall that leads to thrombus formation, which is referred to as septic pelvic thrombophlebitis. This is a life-threatening complication that results in bacteremia and sepsis, which can progress to septic shock and death. Now, surgical wound infections can lead to the formation of an abdominal or pelvic abscess, and in severe cases, necrotizing fasciitis, where the infection involves the subcutaneous tissues and fascia. In the case of cystitis, bacteria can then make their way up the ureters and kidneys, causing pyelonephritis. And finally, mastitis can lead to breast abscess formation.
Okay, so clinical manifestations of postpartum infections generally include chills and a fever with an oral temperature of 100.4° F or 38° C or higher on any two of the first 10 days postpartum; or 101.6° F 38.7° C or higher during the first 24 hours. Other clinical manifestations include malaise, loss of appetite, and tachycardia, with additional signs and symptoms varying based on the type of the infection. So, clients with endometritis usually present with abdominal pain, and foul smelling discharge. The uterus is typically tender and enlarged, due to an inability to return to its normal size after delivery, often referred to as uterine subinvolution. Next are surgical wound infections, where clients experience swelling, tenderness, redness, and warmth of the region. Incisions may sometimes burst open with purulent discharge. Septic pelvic thrombophlebitis should be suspected when the client presents with groin, abdominal or flank pain, along with palpable pelvic veins.