Premature rupture of membranes (PROM): Nursing
1,116views
Premature rupture of membranes (PROM): Nursing
A31- maternal newborn Nursing
A31- maternal newborn Nursing
Notes
| PREMATURE RUPTURE OF MEMBRANES (PROM) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
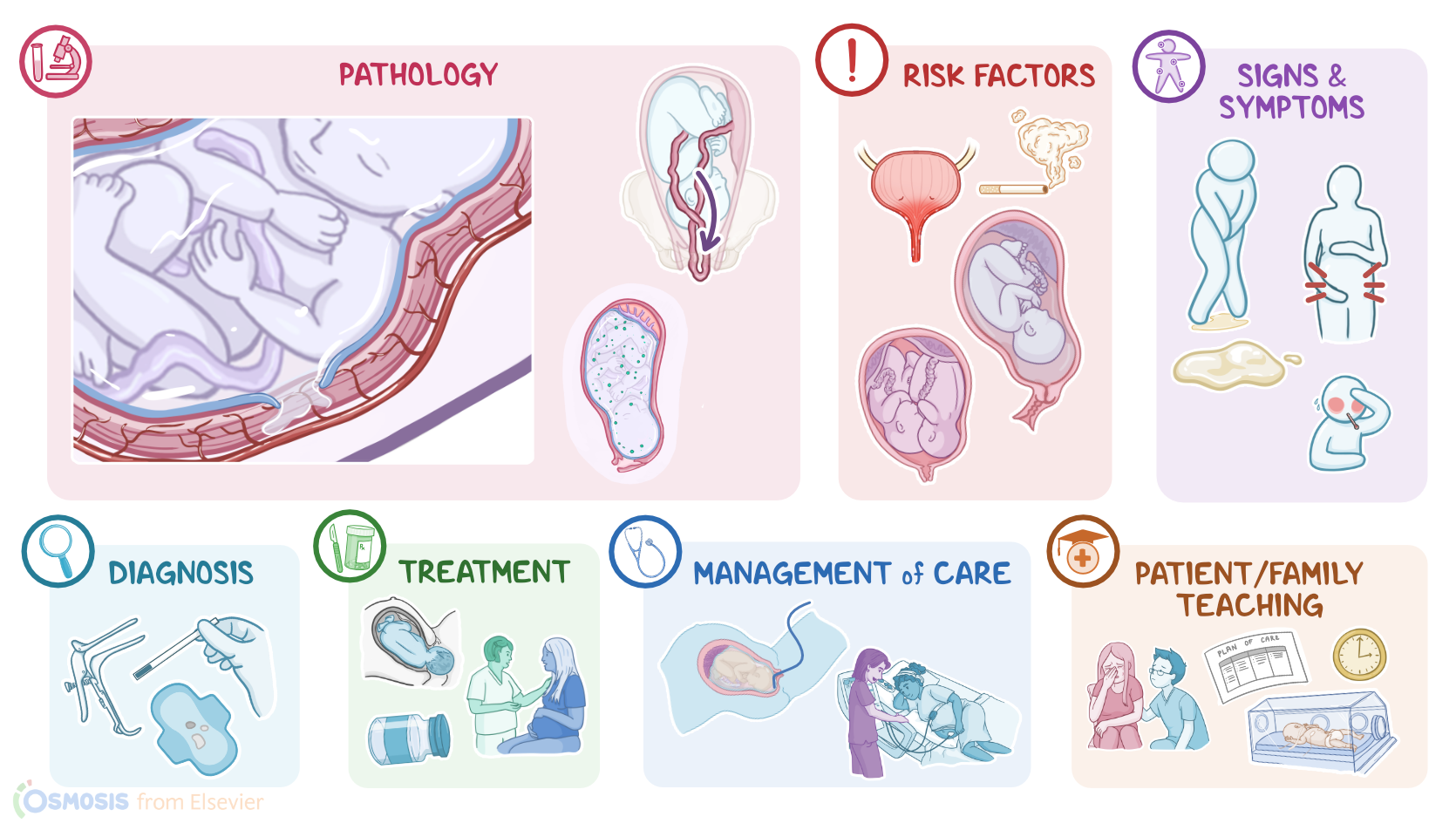
Premature rupture of membranes, or PROM for short, is the rupture of the fetal membranes before the onset of labor. In most cases, this occurs near term, but when membranes rupture before 37 weeks of gestation it is referred to as preterm premature rupture of membranes, or PPROM.
Alright, let’s review some anatomy and physiology. The fetal membranes, also called the chorioamniotic membranes, include the chorion and the amnion. During fetal development, the two membranes fuse together forming the amniotic sac, which is filled with amniotic fluid in which the fetus is suspended. The chorion also forms the fetal part of the placenta, helping in the exchange of nutrients, waste products and gasses between the fetus and the mother. Now, when the amniotic sac ruptures, it releases the amniotic fluid, which is why a lot of people describe it as their “water breaking.” Normally, the rupture of membranes occurs right before the onset of labor and it’s associated with the beginning of uterine contractions.
Although there are several conditions associated with premature rupture of membranes, the exact cause isn’t always clear. Risk factors include a history of PROM or PPROM in a previous pregnancy; genital or urinary tract infections; cigarette smoking; acute abdominal trauma; and uterine overdistention, which can happen as a result of a multiple pregnancy or due to polyhydramnios, which is when there’s too much amniotic fluid inside the amniotic sac.
Now, the pathology of premature rupture of membranes results from a variety of factors that lead to accelerated membrane weakening, eventually causing its rupture. When membrane rupture occurs, a sudden release of amniotic fluid results in oligohydramnios, meaning there’s too little amniotic fluid surrounding the fetus. Premature rupture of membranes is associated with complications like umbilical cord prolapse, which is when the umbilical cord prolapses into the lower uterine segment. In addition,membrane rupture provides a perfect entryway for bacteria to reach the intrauterine cavity, increasing the risk of ascending infections, causing chorioamnionitis, which is when the amniotic sac and fluid get infected. Now, chorioamnionitis is a potentially serious infection, as it can lead to fetal distress, premature labor, or even sepsis.
Alright now, the classic clinical manifestation of PROM is a sudden gush of clear or pale yellow fluid from the vagina, which soaks through the clothes. In some cases, there can be leaking of small amounts of fluid either continuously or intermittently, and sometimes just a sensation of wetness around the perineum. In cases complicated by infection, there may also be fever, tachycardia, a tender uterus, and purulent discharge; as well as fetal tachycardia or decreased fetal movement.
The diagnosis of premature rupture of membranes starts with the client’s history and physical assessment. It’s important to note that digital examination of the cervix should be avoided in cases where PROM or PPROM is suspected, as it can increase the risk of infection, and may precipitate preterm labor. Instead, examination with a sterile speculum can be used to check for fluid pooling in the posterior vaginal fornix.
Once fluid is identified, there are several methods that can be used to verify the fluid is amniotic fluid, such as the nitrazine test, where the nitrazine paper turns blue in the presence of alkaline amniotic fluid; and the fern test, which is when amniotic fluid that’s been dried on a slide makes a fern-like pattern. Other diagnostic tests include certain rapid point-of-care tests to identify substances like alpha fetoprotein and fetal fibronectin in vaginal secretions that indicate membrane rupture.
Now, management of premature rupture of membranes is determined by gestational age, evidence of infection, and evidence of fetal or maternal compromise. Antibiotic prophylaxis is administered regardless of gestational age. Then, if gestational age is between 34 and 37 weeks, labor can be induced with oxytocin. In the setting of PPROM between 24 and 34 weeks of gestation, with no infection or other contraindications to continuing the pregnancy, care involves expectant management with careful monitoring. In addition, since the fetal lungs are not mature at this point, a course of corticosteroids is given to encourage lung maturation. In addition, magnesium sulfate can be given to protect the fetal nervous system if delivery is expected before 32 weeks of gestation. Immediate delivery, on the other hand, is indicated between 24 and 34 weeks when there are signs of intrauterine infection or any other obstetric complications.
Now, if the fetal membranes rupture before 24 weeks, the family should be counseled on poor outcomes for their baby. They could be given the option of immediate induction of labor; or if the mother and fetus are clinically stable, outpatient management can be considered, as long as the mother is able to return to the hospital if bleeding or symptoms of infection occur. In addition, corticosteroids and magnesium sulfate should be administered.
Alright, let’s look at the nursing care you’ll be providing for a client diagnosed with premature rupture of membranes. Your priority goals of care are to promote positive fetal and maternal outcomes and provide emotional support.