Scleroderma: Nursing
Scleroderma: Nursing
Integumentary System
Integumentary System
Notes
| SCLERODERMA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
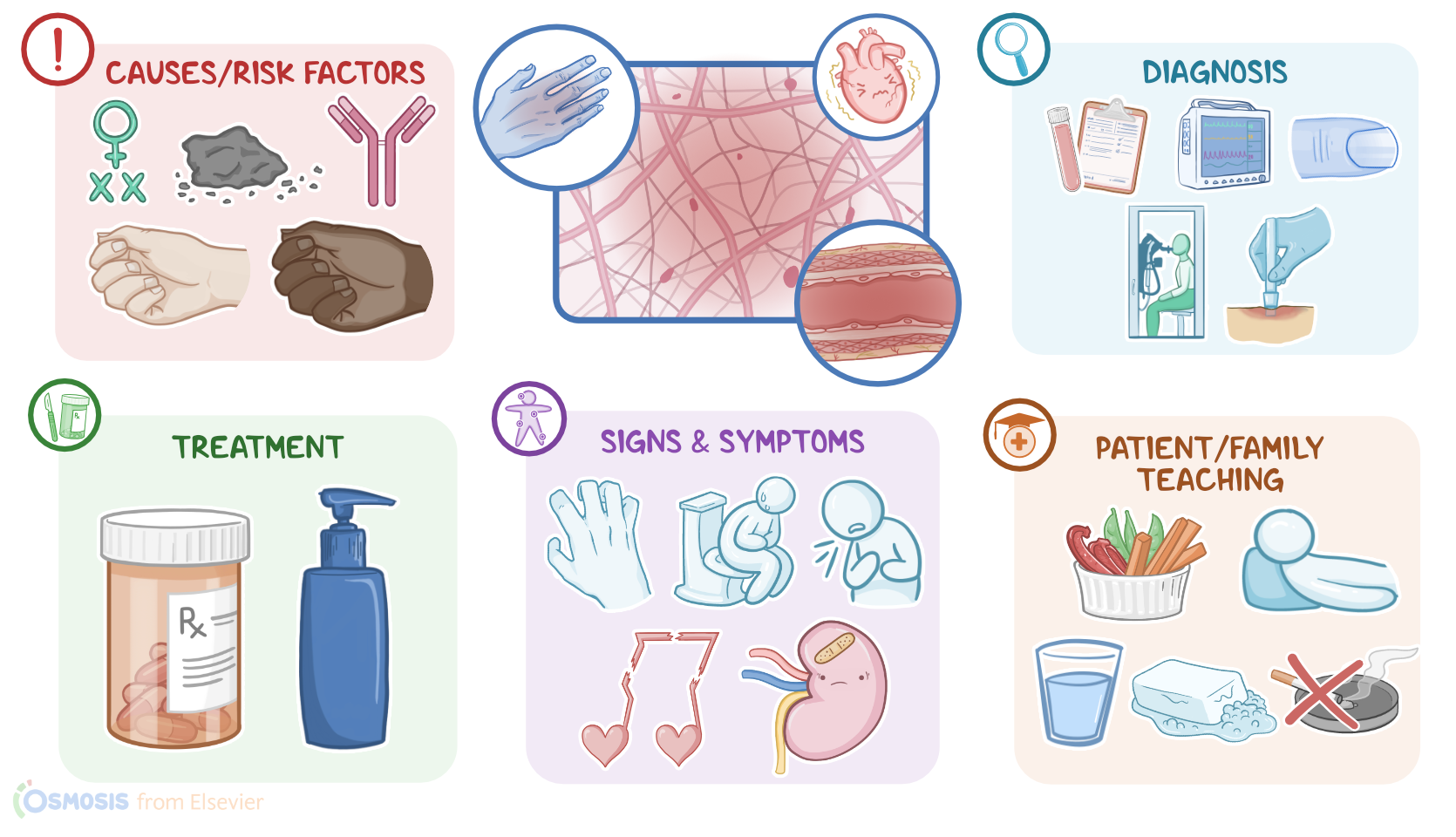
Scleroderma is a connective tissue disease characterized by chronic inflammation, sclerosis, and fibrosis of the skin, blood vessels, and internal organs. There are two types of scleroderma: localized or limited scleroderma, which is more common and typically involves the skin of the face and fingers; and systemic or diffuse scleroderma, which is less common but more severe, as it tends to involve the internal organs too. Let’s start by reviewing the physiology of connective tissue, which is the most abundant tissue type in the body. It provides structural support and protection throughout the body. This tissue houses the most abundant proteins in the body, called collagen, which are large, strong fibers that add elasticity to the connective tissue and helps it in bearing tensile force. Now, the exact cause of scleroderma is still unknown, with some experts suggesting there’s an inflammatory response against the connective tissue. This is often associated with the presence of autoantibodies, namely anticentromere antibodies in localized disease, and topoisomerase-1 antibodies in systemic disease.
Risk factors of scleroderma include being assigned female at birth, in addition to environmental or occupational exposure to coal, plastic, and silica dust. On the other hand, risk factors for localized scleroderma include ages below 40 and white race, whereas risk factors for systemic scleroderma include ages between 30 and 50 and black race. The pathology of scleroderma starts with an inflammatory response that mainly attacks the connective tissue of the skin, blood vessels, and in some cases even internal organs. This causes an increase in the production of collagen fibers, which leads to progressive connective tissue damage and fibrosis. As a result, there’s progressive sclerosis of the skin, as well as microvascular abnormalities and occlusion, and disruption of the normal function of internal organs, mainly the heart, lungs, kidneys, and gastrointestinal tract. Clinical manifestations of scleroderma differ between localized and systemic diseases. Clients with localized scleroderma typically present with CREST syndrome, which stands for calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia.
Calcinosis is a painful deposition of calcium in the skin of the fingers, forearm, and pressure points. Raynaud phenomenon is the most common presentation, and describes decreased blood flow to the fingers caused by brief vasoconstriction of the small blood vessels supplying the fingers due to cold or stress; this results in pallor of the affected fingers, followed by cyanosis or blue discoloration, and finally reactive hyperemia or redness once blood flow is restored. Esophageal dysmotility may present with dysphagia and heartburn. Sclerodactyly refers to the tightening of the skin of the fingers and the toes that doesn’t extend beyond the elbow or the knee. And finally, telangiectasia is characterized by capillary dilation that results in red spots on the skin of hands, forearm, palms, face, and lips. Switching gears, systemic scleroderma usually manifests with rapid and widespread involvement of the skin and internal organs, making it more severe. Clients typically lose skin elasticity, so the skin looks taut, dry, and shiny. This limits joint motion and causes clients to have an expressionless face with tightly pursed lips.
Additionally, there’s reduced temporomandibular joint, or TMJ, motion; sclerodactyly and taut skin around the wrist; lightening or darkening of the skin; as well as loss of limb hair and decreased sweat production. Regarding the internal organs, involvement of the gastrointestinal tract can cause constipation or diarrhea, whereas involvement of the lungs causes cough, dyspnea, pleural thickening, abnormal pulmonary function, pulmonary arterial hypertension, pulmonary fibrosis, and interstitial lung disease. The heart can also be affected, leading to arrhythmias, pericarditis, and pericardial effusion. Lastly, involvement of the renal system causes rapid, progressive, and irreversible renal damage, leading to scleroderma renal crisis, which is characterized by acute renal failure and malignant hypertension. The diagnosis of scleroderma starts with the client’s history and physical assessment. This can be followed by blood tests to screen for anticentromere or topoisomerase-1 autoantibodies. Additional diagnostic tests may depend on the client’s symptoms. An electrocardiogram can be performed to detect cardiac involvement, urinalysis to detect renal involvement, and pulmonary function tests or a chest x-ray may show lung involvement.
Nail bed capillary microscopy can also be done to detect microvascular abnormalities, and in some cases, biopsy of affected skin or organs can help confirm the diagnosis. Unfortunately, there’s no cure for scleroderma, so the treatment aims at relieving symptoms and slowing the disease progression. This can include corticosteroids to ease the clinical manifestations of inflammation, in addition to calcium channel blockers like nifedipine or PDE5 inhibitors like sildenafil for Raynaud phenomenon. Additional treatment options are tailored to the client’s presentation. Okay, let’s look at the nursing care you’ll be providing for a client diagnosed with scleroderma. Your priority nursing goals are to assist in decreasing symptoms and provide psychosocial support. Begin by instituting measures to ease your client’s symptoms. Keep the room at a comfortable temperature to avoid triggering Raynaud phenomenon, and provide gloves to provide warmth, as needed. Then, administer the prescribed calcium channel blocker to promote vasodilation to the extremities.