Prenatal care: Nursing
Prenatal care: Nursing
Gyno, prenatal, pregnanct care
Gyno, prenatal, pregnanct care
Notes
| PRENATAL CARE | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PRECONCEPTION COUNSELING |
| |
| FIRST TRIMESTER |
| |
| SECOND TRIMESTER |
| |
| THIRD TRIMESTER |
| |
Transcript
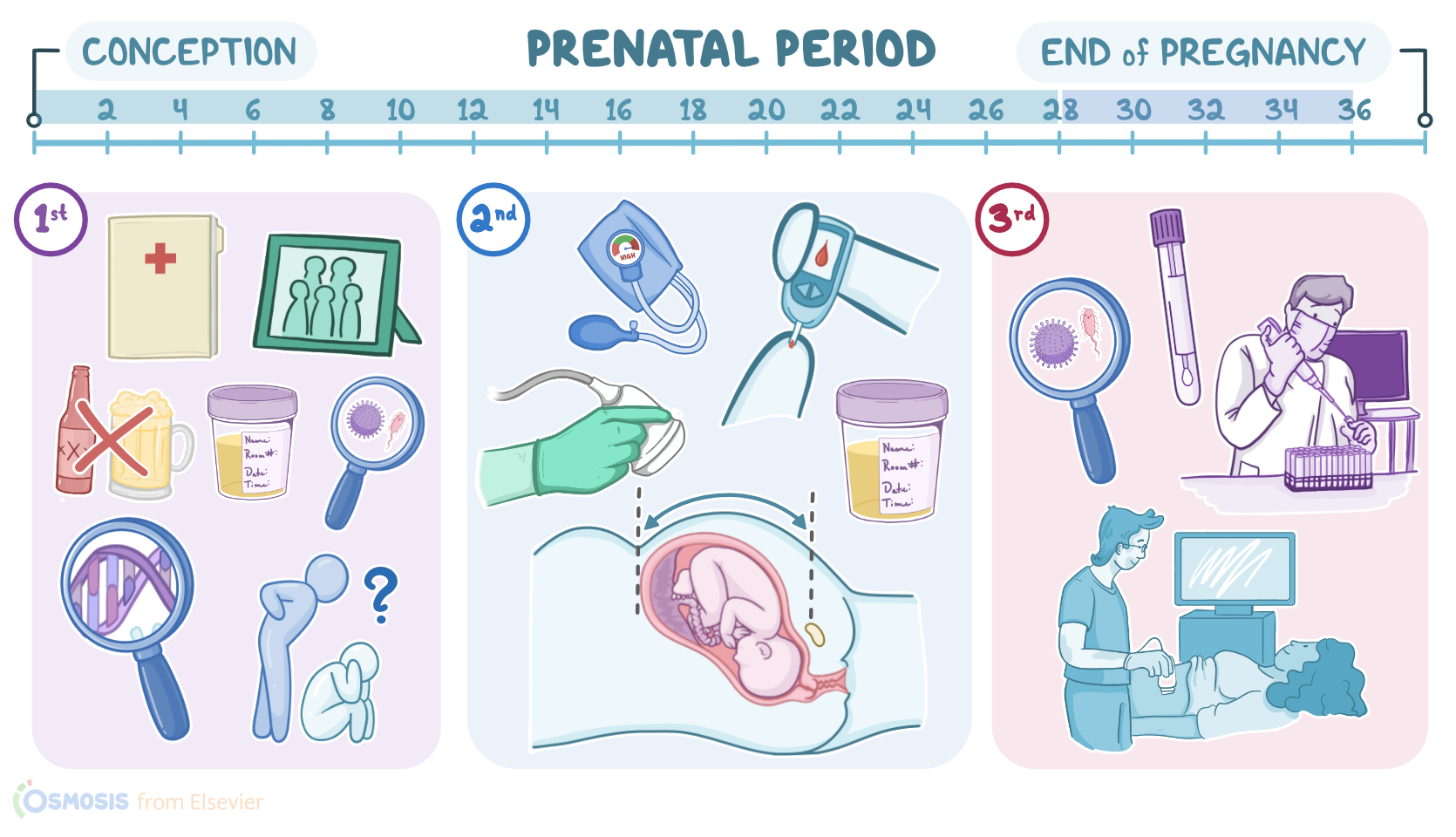
The prenatal period refers to the time from before conception until the end of pregnancy. So, prenatal care refers to the care that is provided before and during pregnancy to evaluate maternal and fetal health, provide education to promote health, and to intervene when possible to ensure the birth of a healthy baby with minimal risk for the mother. For a successful pregnancy outcome, prenatal visits should continue every 4 weeks until week 28, every two weeks from week 28 to 36, and then weekly until delivery.
All right, now the first step in prenatal care is preconception counseling, which seeks to identify any potential risks to the client’s fertility and pregnancy outcome. The first prenatal visit typically occurs when a client suspects they are pregnant or because they wish to conceive in the near future. No matter the case, the main focus of the first prenatal visit should be obtaining a thorough personal and obstetrical history, as well as family history, to identify any medical conditions that could pose a risk to the pregnancy. Now, in clients who suspect they are pregnant, pregnancy should be confirmed with a urine pregnancy test and an abdominal ultrasound. If pregnancy is confirmed, the estimated date of delivery, or EDD, should be calculated. It’s traditionally calculated using Naegele’s rule, which takes the first day of the last menstrual period, or LMP, subtracts 3 months, and then adds one year and seven days. So, if the LMP was September 10, 2021, counting back 3 months, adding 1 year and 7 days calculates the EDD as June 17, 2022.
The obstetrical history evaluates the gravidity, parity, and abortions. Gravidity, or G, refers to the number of times a client has been pregnant, including the current pregnancy. Parity, or P, refers to the number of times a client has carried the pregnancy to a viable gestational age, which is more than 20 weeks gestation. So, if a client is currently pregnant, has been pregnant once before, and has had one viable birth, you’d say that as Gravida 2, Para 1, or G2P1. A more detailed evaluation evaluates Gravidity; as well as the number of Term births at 37 or more weeks of gestation; the number of Preterm births or infants born after 20 weeks of gestation but before completion of 37 weeks of gestation; the number of Abortions, either spotaneous or therapeutic; and the number of children that are currently Living. So, if a client is pregnant for the fifth time, and has 3 children currently alive who were born at term, and had a spontaneous abortion at 16 weeks, the clients GTPAL would be G5T3P0A1L3.
Next, a family history can provide insight about any genetic conditions or disorders that may be passed on to a child. In clients with a family history of genetic disorders, like cystic fibrosis or sickle cell anemia, individuals may benefit from genetic testing to see if they or their partner have the mutation. Genetic screening can also be done to assess the risk of fetal chromosomal anomalies, or aneuploidies, like Down syndrome. Genetic counselling can also be recommended in clients with a history of infertility, multiple spontaneous abortions, or stillbirth; as well as if they’ve had a previous pregnancy or child affected by a birth defect or genetic condition. The rest of the history focuses on identifying any chronic medical conditions that can affect the pregnancy, like diabetes, hypertension, asthma and epilepsy, as well as mental health disorders. Some of the medications used in the treatment of these conditions are known to be teratogenic, and may need to be changed to a less harmful alternative during pregnancy, if possible. Additionally, counseling to stop unhealthy habits, such as smoking, alcohol use, and use of illicit drugs should also be provided. Finally, it’s important to identify any social concerns, such as the possibility of domestic abuse, lack of social support, or economic constraints, any of which can negatively affect the course of a pregnancy.
After completing the medical history, a physical exam and laboratory evaluation should be done. Physical examination focuses on checking the heart, breasts, thyroid, lungs, and abdomen, as well as blood pressure measurement. The body mass index, or BMI, should also be calculated, and the current weight is recorded to keep track of weight gain during pregnancy. Next, the laboratory evaluation consists of determining the client’s blood group and Rh status; hemoglobin, hematocrit, and ferritin levels; as well as screening for infections that could have an adverse impact on the fetus. Screening for infections like HIV, syphilis, chlamydia, and viral hepatitis, is also done, and immunity against diseases like rubella and varicella is documented. Now, during the second trimester of pregnancy, things get a bit more specific. Blood pressure is measured to look for the possible onset of a hypertensive disorder of pregnancy, like preeclampsia. Urine samples are analyzed for asymptomatic bacteriuria or for a urinary tract infection, but it’s also important to look for proteinuria, which is consistent with preeclampsia. In addition, an ultrasound is done at every visit to assess fetal growth, determine any fetal abnormalities, and check amniotic fluid levels. At around 14 to 18 weeks gestation, it is also possible to assess the fetal genitalia for male or female characteristics!