Rubella (German measles): Nursing
Notes
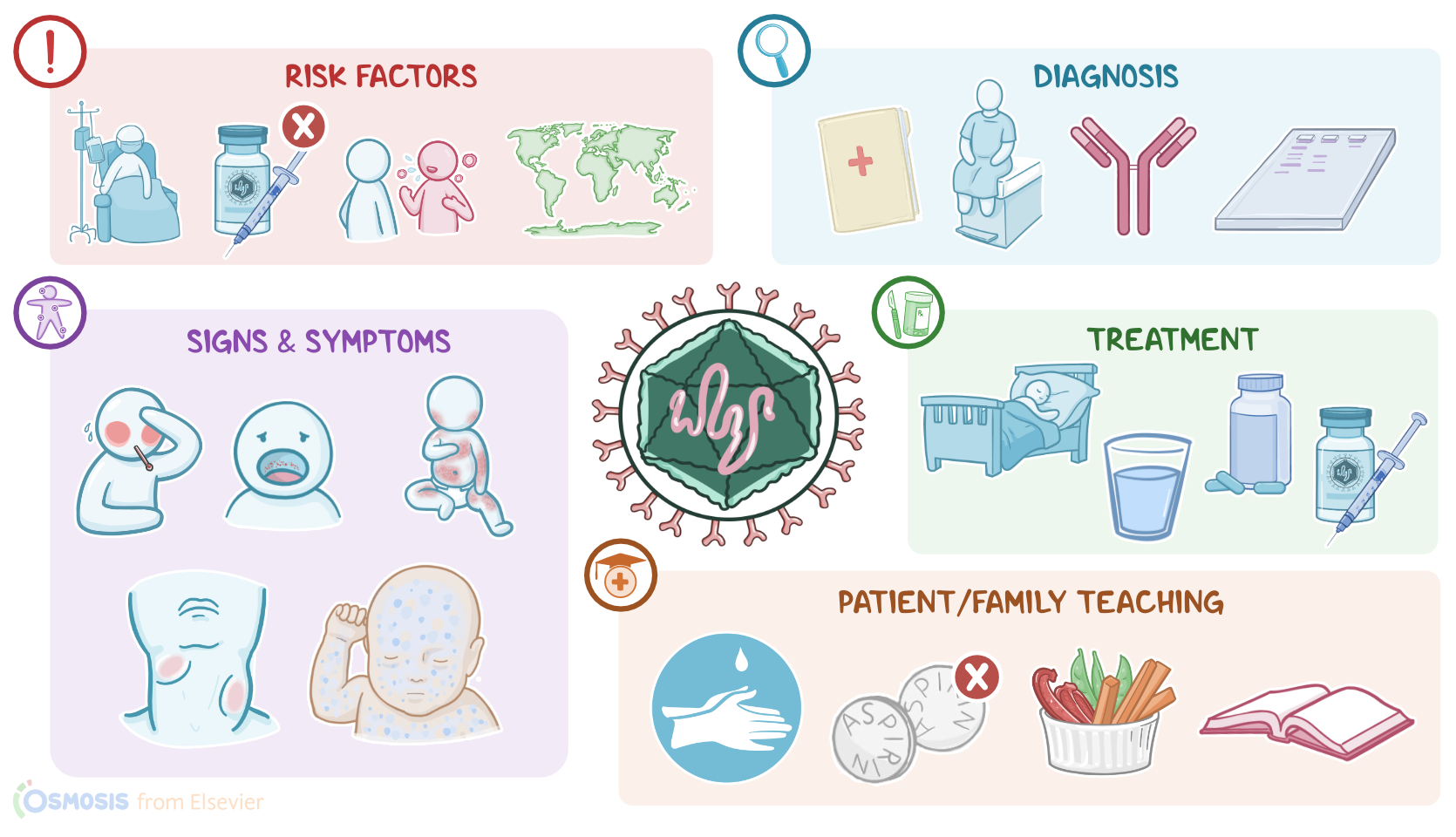
| RUBELLA (GERMAN MEASLES) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Rubella, also known as German measles or the 3-day measles, is a mild viral childhood infection caused by the Rubella virus and is usually associated with malaise, fever, rash, and lymphadenopathy. Thanks to vaccination, there are fewer cases of rubella, but in some parts of the world where the population is not immunized, it’s still possible to see outbreaks.
Now, the cause of rubella is infection with the Rubella virus, which is an RNA virus that has recently been reclassified to the Matonaviridae family from the Togaviridae which it originally belonged to. Important risk factors for rubella include immunodeficiency; being unvaccinated or incompletely vaccinated; coming in contact with an infected person; and finally, living in or traveling to an endemic area.
Moving on to pathology. Rubella virus is an airborne virus, meaning it spreads via small virus-containing droplets that get flung in the air when an infected person coughs or sneezes. If another person breathes in these droplets, or they get in contact with infected surfaces and then touch their mouth, nose, or eyes, they can become infected.
Once the virus enters the body, it binds to a specific receptor on the membrane of epithelial cells in the nasopharynx and enters the cell. Inside the cell, the virus replicates, creating new viral particles, which leave the cell and enter surrounding lymphatic and blood vessels, eventually reaching regional lymph nodes where they replicate once again. From here, the virus enters blood vessels again, and spreads throughout the body, making its way into various bodily fluids like urine, cerebrospinal fluid, and synovial fluid of joints. Important complications of rubella infection include polyarthritis and polyarthralgia.
Now, the virus can also cross the placenta during pregnancy, causing congenital rubella syndrome, or CRS for short, in the fetus. The risk of CRS is highest when the pregnant individual gets rubella during the first trimester. Infection during this time can lead to a triad of problems that include sensorineural hearing loss; cataracts; and congenital heart defects. CRS can also result in miscarriage, stillbirth, low birth weight, hemolytic anemia, and microcephaly. In fact, rubella is among the most common infections that cause congenital defects in fetuses, which are grouped under the acronym TORCH. T stands for Toxoplasmosis, O for Other infections like Syphilis, R for Rubella, C for Cytomegalovirus, and H for Herpes Simplex.
Now, infection with the rubella virus is often asymptomatic. After exposure, there’s an incubation period of 12 to 23 days, which is often followed by prodromal symptoms, including a low-grade fever, sore throat, mild conjunctivitis, and general malaise; along with petechiae, which can be noted on the the soft palate. Then, maculopapular rash appears during day 14 to 17, which is made up of little pink or light red macules and papules that start on the face and spread downward to the trunk and extremities.
The lesions are usually discrete; but they can become more obvious after a hot shower or bath. The rash can also be accompanied by itching or minimal desquamation and it usually clears up in 2 to 4 days. It’s important to note that shedding of the virus is likely happening 5 days before the rash appears and 6 days after the rash resolves, so this is when individuals with rubella are most likely to spread the virus to other people.
Other clinical features include symptoms of upper respiratory tract infection, like cough, and runny nose, as well as regional lymphadenopathy, or swelling of posterior cervical, postauricular, and occipital lymph nodes. Finally, neonates born with CRS can have a characteristic “blueberry muffin” rash, characterized by numerous reddish-blue purpuric papules and macules.
Diagnosis of rubella is typically based on the client’s history, and physical assessment, followed by detection of rubella-specific IgM antibodies, which indicate current infection. Additionally, a PCR test can be used to detect viral RNA in amniotic fluid, fetal blood, or chorionic villi.