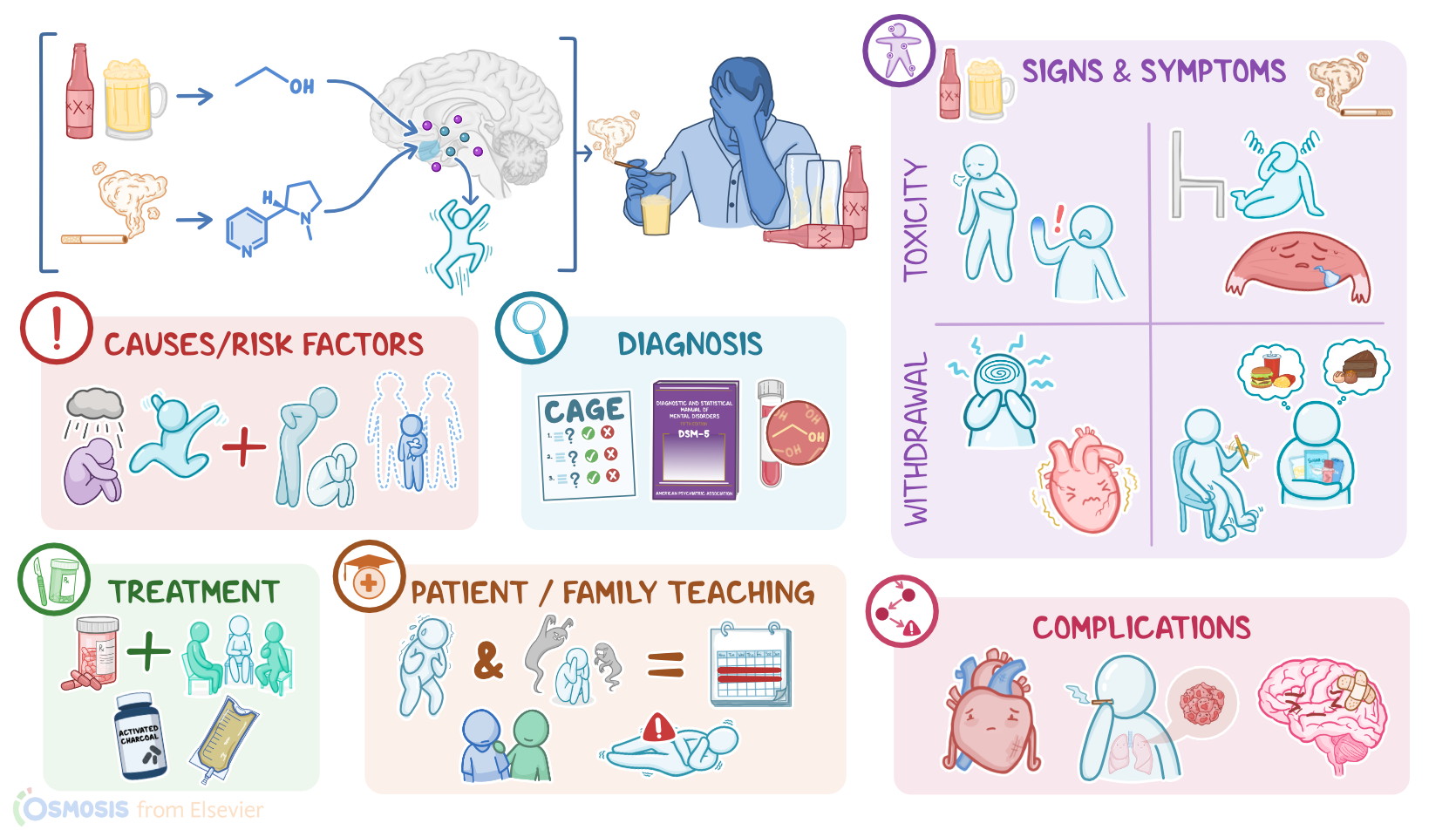
Substance use disorder - Alcohol and tobacco: Nursing
Notes
| SUBSTANCE USE DISORDER - ALCOHOL & TOBACCO | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Substance use disorder is a condition in which an individual is unable to control their use of legal or illegal substances. Some of the most commonly used substances include alcohol and tobacco. There are three different stages of substance use: dependence where the substance is repeatedly used, tolerance where an increased amount of the substance is needed to have the same effect, and addiction where the substance use is recurrent and uncontrolled.
Okay, let’s quickly review the physiology of the brain’s reward center. Inside the brain are small molecules called neurotransmitters that are produced and used by neurons to communicate with each other. This communication happens when one neuron releases a neurotransmitter which then binds to the receptors of another neuron causing the neuron to react.
Now, in the rewards system, dopamine is the primary neurotransmitter. And so, when a person experiences pleasure, a surge of dopamine is released from the nucleus accumbens, which is a cluster of nerves near the hypothalamus, more commonly known as the brain’s reward center.
Now, there isn’t a single cause of substance use disorders, but rather it’s a multifactorial disease, meaning that there’s a combination of genetic predisposition and environmental risk factors and triggers. These include a family history of substance use disorder or having a mental health disorder like depression, ADHD, or PTSD. Certain experiences also put a client at high risk for developing a substance use disorder like using the substance at an early age, or experiencing physical, sexual, or emotional abuse.
Okay, so the pathology of substance use disorder centers around the fact that alcohol contains ethanol, while tobacco contains nicotine. Both can trigger the release of dopamine and other neurotransmitters in the brain and create a pleasant and euphoric feeling when using the substance. This in turn motivates the client to repeatedly use the substance.
It’s important to note that not everyone who uses a substance develops substance use disorder, for example someone who’s given morphine in the ER for kidney stones. A substance use disorder develops when long term use of a substance leads to severe physical, psychological, or social impairment in the client.
One reason this occurs is due to the body developing tolerance to the substance with chronic use. This is where neurons adapt to the dopamine over exposure by producing less and less dopamine or reducing the number of dopamine receptors. This lessens the effect of the substance so that the client needs to consume more and more of it to get the same euphoric feeling.
And at the same time, the natural response of dopamine release from other enjoyable experiences also becomes so low that the only way to start feeling happy again is using the substance and this is called dependence. At this stage, if the client stops using the substance they may suffer physical and mental withdrawal symptoms.
Each type of substance can also affect other parts of the body. So, chronic alcohol use can damage blood vessels, causing hypertension, coronary artery disease, or stroke, as well as the heart, causing arrhythmias, and dilated cardiomyopathy. Chronic alcohol usage can also damage liver cells, or hepatocytes, affecting their ability to function, and leading to alcoholic liver disease. This is characterized by liver damage and fat build up which is called steatosis, and this can lead to cirrhosis. Similarly it can cause pancreatitis, and damage parts of the GI tract, causing peptic ulcers, and GI bleeds.
It’s also common to see vitamin deficiencies in those with chronic alcohol use, largely thought to be due to having a poor diet. An example is vitamin B1 or thiamine deficiency, which can lead to Wernicke’s encephalopathy.
Alcohol use is also associated with the risk of developing certain cancers, including mouth, throat, esophagus, liver, and breast cancer. Finally, alcohol’s effect on the brain can also lead to dementia, depression, and anxiety.
Likewise, smoking tobacco can damage the lungs and blood vessels which can eventually cause chronic obstructive pulmonary disease, lung cancer, as well as stroke, hypertension, heart disease, or even a heart attack. The use of chewing tobacco can cause periodontal disease and cancers from the mouth to the esophagus.
Electronic cigarettes may also affect the respiratory, immune, and cardiovascular systems, and may even alter brain development in adolescents or embryos of clients who are pregnant.
Alright, so the clinical manifestations of substance use disorders in general often include a lack of energy, weight loss or gain, and changes to behavior like needing the substance daily, intense urges for the substance, and using the substance even if it causes harm. The client may appear unkempt and may begin missing school or work or any other regular activities.
Now, when a client experiences acute alcohol toxicity, they can present with behavior changes like agitation, anxiety, confusion, and slurred speech. In addition, they can experience vomiting, slow or irregular breathing and even be unresponsive, in a coma, or cyanotic.
Now, symptoms of tobacco toxicity may initially be stimulatory, and include excessive salivation, sweating, hypertension, tachycardia, tachypnea, headache, dizziness, muscle fasciculations, tremor, and seizures. This might be then followed by a period of depressor effects, including hypotension, bradycardia, difficulty breathing, slurred speech, coma, and muscle weakness.
Now, clients with alcohol or tobacco use disorder can present with withdrawal symptoms when they abruptly stop drinking alcohol or using tobacco. Symptoms of alcohol withdrawal include anxiety, irritability, hypotension, tachycardia, tremors, and seizures. A severe complication of alcohol withdrawal, called delirium tremens, can present with high fever, tachycardia, hypertension intense agitation, visual or auditory hallucinations, and even tactile hallucinations where it feels like something is crawling on the skin. If left untreated, delirium tremens can lead to seizures and even death.
An important tool for evaluating the severity of withdrawal is The Clinical Institute Withdrawal Assessment of Alcohol Scale, or CIWA-Ar. It looks at the severity of anxiety, sweating, nausea and vomiting, visual, auditory and tactile hallucinations, headaches, and tremors.
Now, symptoms of tobacco withdrawal include severe craving for tobacco, anxiety, irritability, anger, poor concentration, restlessness, impatience, increased appetite, weight gain, and insomnia.
Diagnosis of substance use disorder begins with the client’s history and physical assessment, followed by a CAGE questionnaire where four brief yes or no questions are used to check for signs of possible alcohol dependency. The four questions are; “Have you ever felt you should cut down on your drinking?” “Have people annoyed you by criticizing your drinking” “ Have you ever felt bad or guilty about your drinking?” and “Have you ever had an eye opener, or drink first thing in the morning to steady your nerves or to get rid of a hangover”
Diagnosis is confirmed using the Diagnostic and Statistical Manual for Mental Disorders fifth edition or DSM-5 criteria, which is a set of diagnostic criteria indicating the symptoms that must be present, and for how long, to diagnose substance use disorder. Finally, blood alcohol concentration may also be checked.
Treatment for alcohol and tobacco use disorder usually involves a combination of psychotherapy and pharmacotherapy. There are several types of psychotherapy, including cognitive behavioral therapy, motivational enhancement therapy, group therapy such as self-help groups like Alcoholics Anonymous, and family therapy. These focus on teaching the client strategies to better cope with stress and social pressures, as well as to identify the thoughts, feelings, and behaviors that lead to substance use, and create a plan to navigate triggers for use. In addition, clients may benefit from lifestyle modifications like physical activity, yoga, meditation, deep-breathing exercises, and acupuncture.
Regarding pharmacotherapy for alcohol use disorder, disulfiram or naltrexone can help make drinking alcohol less rewarding. For tobacco use disorder, nicotine replacement therapies can help a client slowly taper off from their regular dose of nicotine and ultimately quit altogether. These include nicotine-containing gum, lozenges, transdermal patches, nasal sprays, inhalers, dissolvable tobacco, mouth sprays, and sublingual products.
Now, more extensive support and treatment is required for acute alcohol or tobacco intoxication or withdrawal. So, for acute alcohol intoxication, after making sure that the ABCs, or airway, breathing, and circulation are maintained, it is important to administer IV fluids, glucose, as well as vitamin B1, to prevent complications like Wernicke-Korsakoff’s syndrome. For tobacco intoxication, activated charcoal might be administered to decrease gastrointestinal absorption.
For clients going through withdrawal from alcohol, treatment involves benzodiazepines, such as chlordiazepoxide, lorazepam, or diazepam, which act as central nervous system depressants, as well as IV fluids, vitamins, and glucose, which are often called a “banana bag” when given together.
On the other hand, those with tobacco withdrawal are often given bupropion or varenicline, which help reduce withdrawal symptoms and prevent relapse.