Anemia - Aplastic: Nursing
1,509views
Anemia - Aplastic: Nursing
Watch later
Watch later
Notes
| ANEMIA - APLASTIC | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
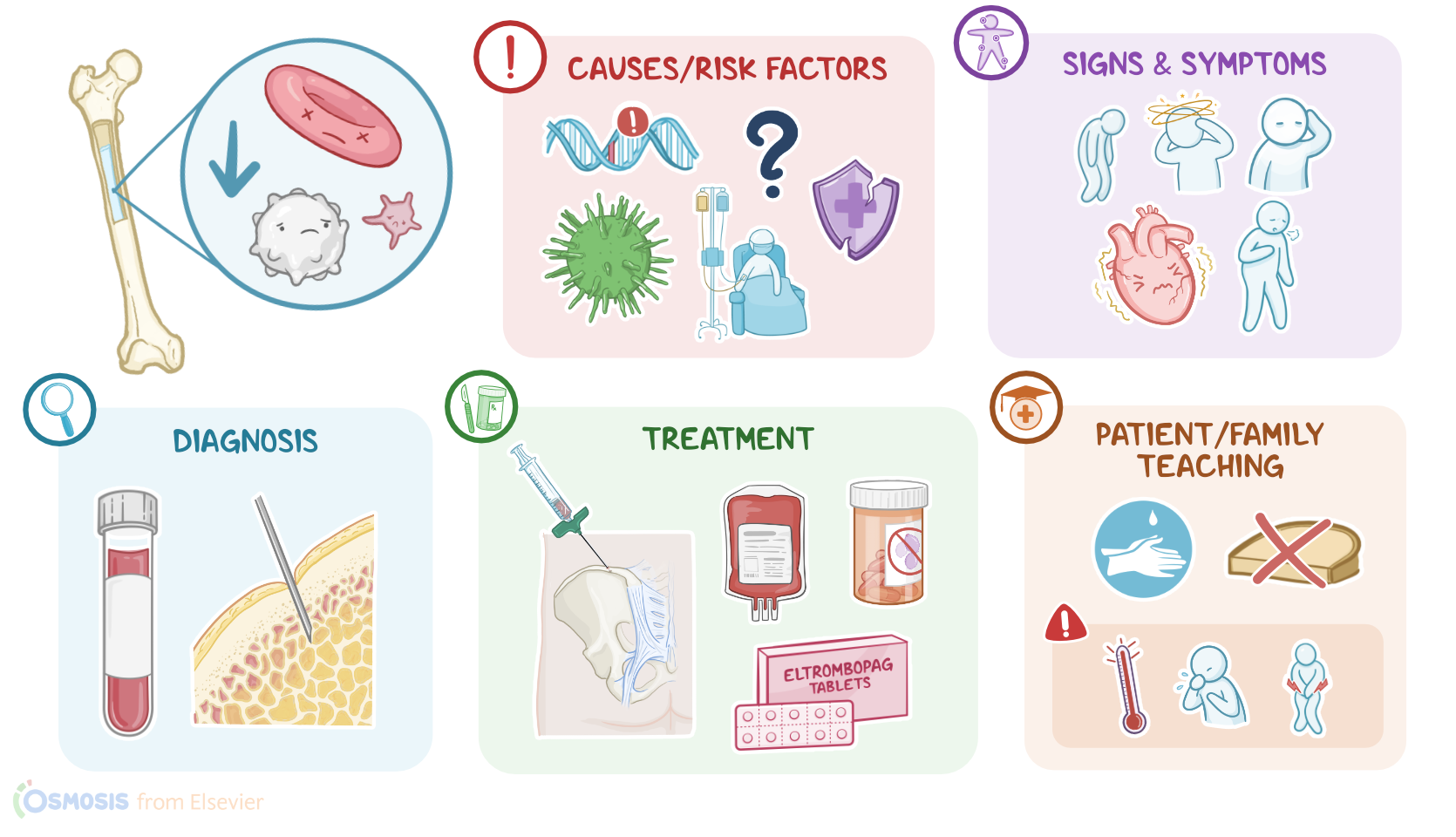
Aplastic anemia is a condition characterized by pancytopenia, meaning decreased production of all blood cell lines, so red and white blood cells, as well as platelets. This condition can be inherited, when it occurs because of genetic mutations, as well as acquired, when it occurs because of external factors.
Let’s start by looking at the physiology of blood cell production, or hematopoiesis. This process starts in the bone marrow, which is the innermost portion of bone, where hematopoietic stem cells reside. These serve as progenitor cells for all the different cell types found in the blood, including white blood cells, which primarily function as the defense mechanism against infections; as well as red blood cells, which are essential to carry oxygen to the tissues; and platelets, which play a key role in blood clotting.
Now, hematopoietic stem cells reach their final, mature form, when they receive the appropriate signals in the form of specific growth factors or stimulating factors. One of these growth factors is called erythropoietin, or EPO. This is a hormone released by the kidneys, that tells hematopoietic stem cells to differentiate into red blood cells. Another important factor is the granulocyte colony-stimulating factor, or G-CSF, which is produced by various cells and tissues, including the bone marrow itself, and it stimulates the production of a specific group of white blood cells called neutrophils. Finally, there’s thrombopoietin, a hormone produced by the liver and kidneys, which stimulates platelet production.
Alright, now the causes of aplastic anemia can be inherited or acquired. The most common cause of inherited aplastic anemia is Fanconi’s anemia, a rare genetic disorder characterized by progressive bone marrow failure.
On the other hand, acquired causes of aplastic anemia include any other factor that leads to suppression or destruction of the bone marrow, including other conditions like an autoimmune disease, or undergoing treatments like chemotherapy or radiation therapy. Additionally, many cases are idiopathic, meaning the exact cause is unknown.
Some medications can also cause bone marrow suppression, like antiepileptics such as anticonvulsants hydantoins or carbamazepine; antithyroid medications like propylthiouracil and methimazole; and certain antibiotics like chloramphenicol and sulfonamides.
There are also toxic chemicals associated with bone marrow destruction, like benzene and certain solvents. And last but not least, some viruses like EBV, HIV or hepatitis viruses can also be a cause.
Okay, so the pathology of aplastic anemia starts with an inherited defect or acquired damage to the bone marrow. In most cases, this triggers an autoimmune reaction that destroys hematopoietic stem cells, followed by subsequent replacement of the bone marrow by non-functional fatty tissue. Eventually, clients with aplastic anemia do not have enough hematopoietic stem cells to generate appropriate amounts of mature blood cells, and the end result is pancytopenia.
Now, clinical manifestations of aplastic anemia vary depending on the disease severity. A low red blood cell count can lead to fatigue, dizziness, and pallor. In severe cases, tissues cannot properly oxygenate, so the heart pumps harder to circulate the blood, which can lead to tachycardia, chest pain, and dyspnea.
Next, a low platelet count can lead to increased risk of bleeding due to minor injuries; as well as spontaneous mucosal bleeding, like epistaxis and bleeding gums; and petechiae, which are tiny red spots that appear on the skin because of broken capillaries.
Finally, low white blood cell count predisposes clients to develop recurrent or severe infections.
The diagnosis of aplastic anemia starts with the client’s history and physical assessment; followed by laboratory tests, including complete blood cell count that shows pancytopenia. Usually, the absolute neutrophil count, or ANC is less than 500/mm3, while platelet number is lower than 20,000/mm3. Other common findings include a hemoglobin level below 10g/dL and a decreased number of immature red blood cells, or reticulocytes, which demonstrates decreased red blood cell production; as well as increased levels of EPO, in an attempt to compensate and ramp up the production of red blood cells. In addition, bleeding time may also be increased.
Definitive diagnosis of aplastic anemia requires a bone marrow biopsy, which demonstrates profoundly low counts of hematopoietic stem cells with increased fat content, while at the same time ruling out other causes of bone marrow suppression, like malignancy or fibrosis.
Treatment of aplastic anemia depends on the cause, and can vary depending on the client's age and clinical history. If the condition is thought to be due to a medication or toxic agent, they should be removed immediately.
Supportive treatment includes blood transfusions to correct the anemia and antibiotics, as well as antifungal and antiviral medications to prevent or treat infections.
Key Takeaways
Aplastic anemia is a rare blood disorder caused by bone marrow failure to produce new blood cells. Even though it's referred to as aplastic anemia, it typically presents with pancytopenia, meaning that all three major blood cell lines - the red blood cells, white blood cells, and platelets are affected.
People with aplastic anemia may experience fatigue, shortness of breath, ecchymoses and mucosal bleeding, and frequent infections pallor Aplastic anemia can be caused by a variety of factors, including exposure to radiation or chemotherapy, viral infections, and autoimmune disorders.