Arrhythmias - Premature atrial contractions (PACs): Nursing
Arrhythmias - Premature atrial contractions (PACs): Nursing
Adult Nursing 1 AAS
Adult Nursing 1 AAS
Notes
| ARRHYTHMIAS - PREMATURE ATRIAL CONTRACTIONS (PACs) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Arrhythmias are irregular heartbeats that occur due to any disturbance in the rate, rhythm, site of origin, or conduction of the cardiac electrical impulse, which can affect the heart’s ability to pump blood throughout the body. Premature atrial contractions, or simply PACs, are a type of arrhythmia, where an extra beat starts in a point in the atrium other than the sinoatrial node, and causes the atria to contract earlier than normal in the cardiac cycle.
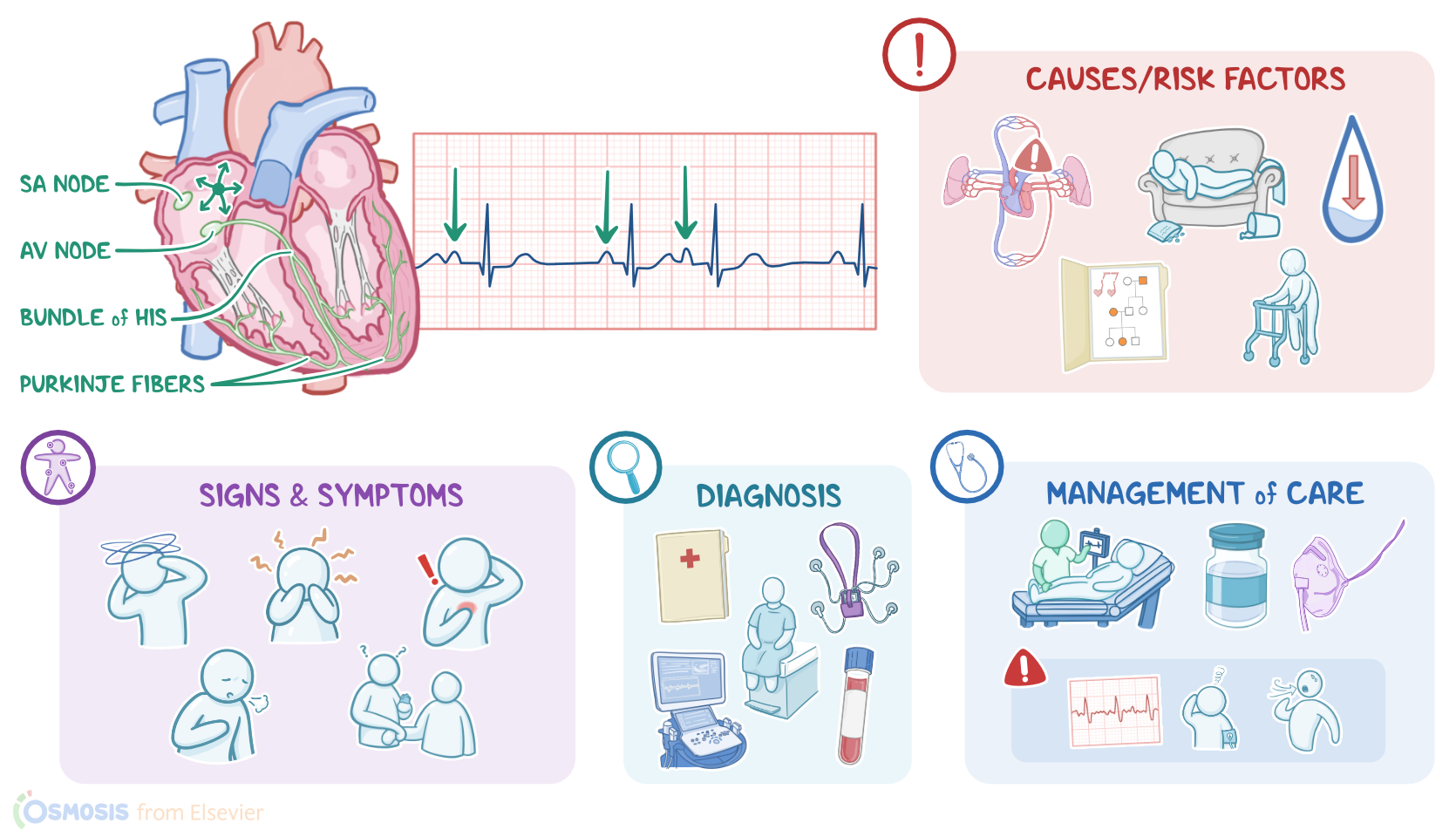
Now let’s look at the normal electrical conduction pathway in the heart on an ECG, which shows how the depolarization wave flows through the heart during each heartbeat. The normal electrical activity of the heart starts in the sinoatrial or SA node, which is considered the pacemaker of the heart. Then, the impulse is conducted through the atrium, creating the P wave on an ECG. And when the atrial muscle cells get depolarized, they contract, pushing blood from the atria into the ventricles. From the atrium, electrical activity goes to the atrioventricular, or AV node, where the impulse propagation speed slows way down; this is the PR interval on an ECG. This pause allows the atria to contract while the ventricles fill with blood. From the AV node, the depolarization wave goes through the Bundle of His, then the right and left branches of the Bundle, and finally through the Purkinje fibers, which deliver the current to the right and left ventricles, causing them to depolarize. This triggers simultaneous contraction of both ventricles, pushing blood into the systemic and pulmonary circulations, and it’s represented by the QRS complex on an ECG. Finally, the ventricles repolarize to prepare for the next cycle, which allows them to relax and fill with blood, called diastole. And on ECG, ventricular repolarization will create a T wave, while the pause between ventricular depolarization and repolarization is represented by the ST segment. Sometimes, immediately after the T wave, there’s a U wave, which represents late repolarization of the ventricles.
Now, the main cause of PAC is irritability of atrial tissue, which is typically idiopathic, meaning we don’t know what causes it. What we do know, though, is that with PAC, an atrial cell outside of the SA node initiates a depolarization, and that’s called an ectopic atrial focus. This signal travels through the walls of the atria, causing them to contract prematurely. In some cases this can be caused by enhanced automaticity, which means accelerated rate of electrical impulse generation. This can happen when atrial cells are irritated and stressed by electrolyte imbalances. Or with damage to cardiac tissue like myocardial infarction, hypoxia from lung diseases like COPD, as well as anything that increases sympathetic activity, like anxiety, emotional stress, and substances like caffeine or nicotine. Another type of atrial ectopic focus is a reentrant loop, which is when some atrial tissue doesn’t depolarize right, this could be due to something like scar tissue from a previous myocardial infarction. As a result the depolarization wave ends up circling around and around that tissue. A reentrant loop basically starts sending out depolarization waves to the rest of the heart tissue each time the wave goes around.
Risk factors can be modifiable or non-modifiable. Modifiable risk factors include lung and cardiovascular disease, sedentary lifestyle, poor sleep, dehydration, and taking certain substances and medication like epinephrine, sympathomimetics, and amphetamines.On the other hand, non-modifiable risk factors include family history of arrhythmias, advanced age, and white race.
Now, whatever the cause of the premature atrial contractions, the pathological process involves disruption of the normal heart rhythm. The impulse from the ectopic focus travels through the walls of the atria causing a contraction. At the same time, the signal depolarizes the cells of the SA node, which causes the SA node to skip a cycle of sending its own signal, causing a reset. Now, when the depolarization wave gets to the AV node, there are a few things that could happen. If the AV node has recovered from its previous refractory period, the signal may pass normally through the AV node and into the ventricles, causing them to contract. Alternatively, the signal might get through the AV node but have trouble getting sent through the ventricles, like when the right bundle branch has not recovered from its own refractory period. In this situation, the depolarization wave conducts down the left bundle branch and then through the ventricles aberrantly. Finally, if the signal arrives at the AV node while it's still in the refractory period, it might either get delayed or stop completely, and not get conducted to the ventricles, so there will be no ventricular contraction. These are called non-conducted PACs.
PACs are typically isolated events. If they keep happening though, especially in clients with an underlying heart disease, they can lead to serious complications, including heart failure. That’s because, with recurrent PACs, the heart won’t have time to fill with as much blood as it normally would, so there won’t be as much blood to pump out. At the same time, less blood is delivered to the brain, which can lead to ischemic stroke. Finally, in rare cases, an ectopic focus can trigger atrial flutter or atrial fibrillation, which are more serious arrhythmias where the atria essentially just quiver instead of effectively pumping blood into the ventricles.
Clients with PACs are typically asymptomatic, while some clients present with dizziness, lightheadedness, and anxiety. Clients might also experience palpitations, or feel like their heart skips a beat. In cases of heart failure, clinical manifestations may also include shortness of breath, tachypnea, orthopnea, in addition to decreased urine output, delayed capillary refill, and jugular venous distention, or JVD for short.
Upon palpation of peripheral pulses, rhythm irregularities might be found, whereas auscultation of the heart may reveal early or additional heart sounds, in addition to a pause in the heart’s rhythm.
The diagnosis of PACs starts with the client's history, and physical assessment, followed by the use of a Holter monitor, which is basically a portable ECG that records for a 24-hour period. So, on the ECG heart rate may vary, rhythm is irregular, and the P waves are abnormally shaped, because they originate outside the SA node. And because they occur earlier than expected, they might happen at the same time as the T-wave from the previous, normal contraction. In this case, the two waves will combine, making that T-wave look peaked, or more lumpy than usual, kind of like a camel’s hump. PR intervals might be shorter than usual when the ectopic focus is close to the AV node, or longer than usual if there’s a delay in the AV node. The QRS complex is typically normal, meaning that the signal passes normally through the AV node and into the ventricles. On the other hand, a QRS complex that's wider than normal, meaning longer than 0.12 seconds, means that there’s abnormal conduction through the bundle branches and into the walls of the ventricles. Alternatively, the P wave might not be followed by a QRS complex at all, in the case of a non conducted PAC. Finally, a compensatory pause might be seen after a normal cycle, if the signal gets to the SA node and causes it to skip a beat.