Burn injury: Nursing
Notes
| BURN INJURY | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
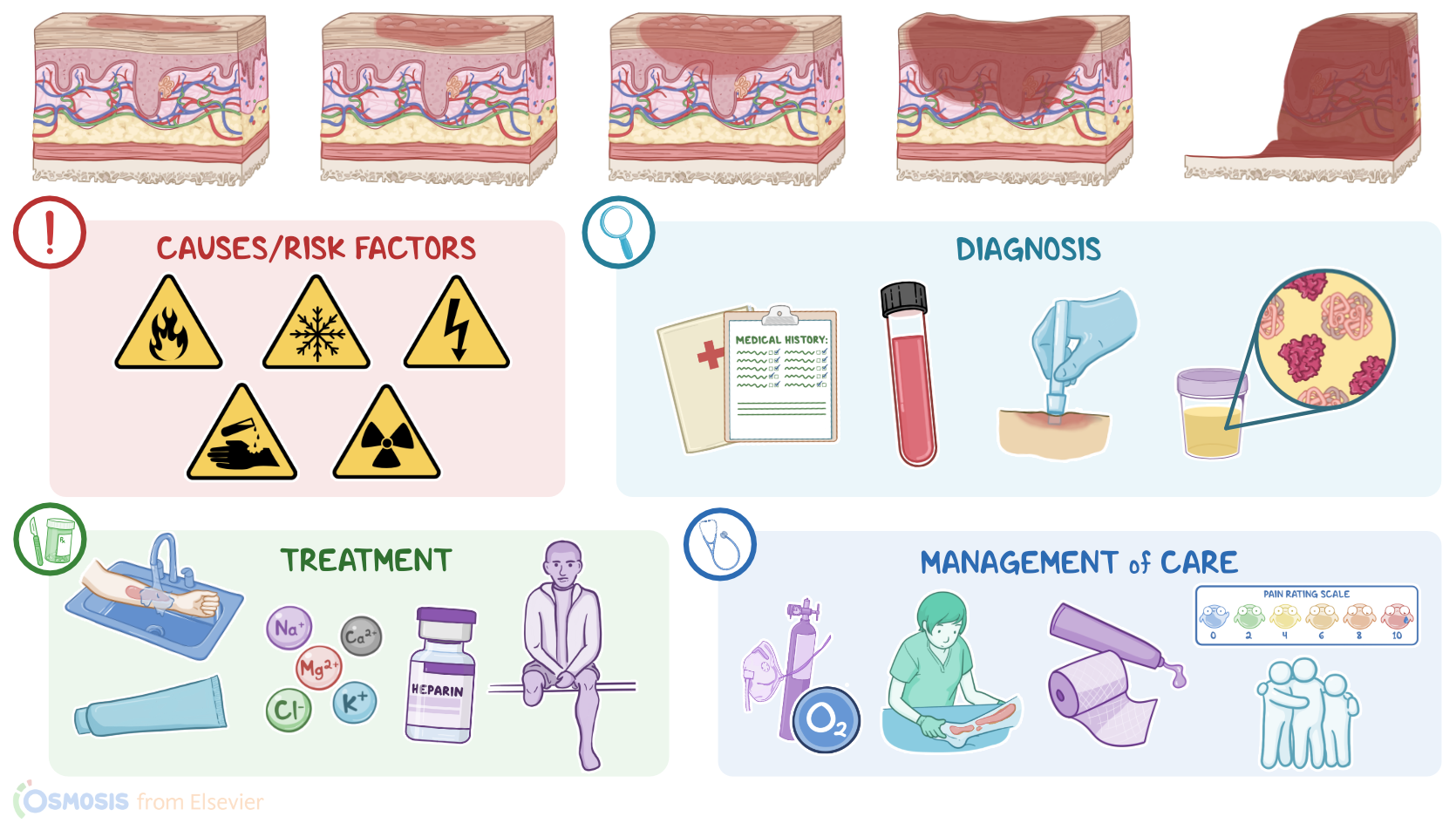
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEAHING |
| |
Transcript
Burn injuries are a type of acute wound where the skin and tissue underneath are damaged by exposure to heat, extreme cold electricity, chemicals, or radiation.
Okay, first, let’s talk about physiology. The skin is the outer barrier that protects the body from excessive water loss, as well as any external threat like pathogens. The skin is divided into three main layers, the hypodermis, dermis, and epidermis. The hypodermis is made of fat and connective tissue that anchors the skin to the underlying muscle and acts as a cushion that protects underlying tissues from trauma. Above the hypodermis is the dermis, which is made of proteins like collagen that provides structural support, as well as elastin that provides flexibility. The dermis also contains hair follicles, nerve endings that collect sensory information, as well as sweat glands, and blood vessels, which help regulate body temperature. And just above the dermis is the epidermis, which itself has multiple cell layers that are composed of developing cells called keratinocytes.
Now, the skin has this special ability to repair itself when damaged. To do that, there are three main processes: reepithelialization, granulation, and wound retraction. Reepithelialization describes the resurfacing of damaged skin by new skin cells. If the damage is too great to be fixed only by reepithelialization, granulation and wound retraction come into action. Granulation is the process of forming granulation or scar tissue, which contains new blood vessels and fibroblasts. These fibroblasts form new connective tissue and have the ability to contract, pulling the edges of the wound together in a process called wound retraction.
Okay, burn injuries can be classified based on the cause. The most common cause are thermal burns, which can result from scalds from hot liquids or steam, from open flames, such as from house fires, or by direct contact when a hot object like oven doors or cookware is touched. Less commonly, there’s electrical burns from exposure to a lightning strike or high-voltage electrical current, and chemical burns from exposure to chemical substances like acid or alkaline chemicals. Finally, there’s radiation burns, which can be caused by exposure to UV radiation from the sun or from radiotherapy.
Alright, now burn injuries can also be classified based on the degree, depending on the severity. Starting with first degree burns, these are also called superficial burns and involve the epidermis only. Next are second degree burns, which are further classified into superficial second degree burns, which involve the epidermis and the superficial dermis; and deep second degree burns, which also involve the deeper parts of the dermis. Third degree burns are full-thickness burns, destroying the entire epidermis and dermis. Finally, fourth degree burns, also called deep full-thickness burns, extend beyond the dermis, destroying deeper structures like muscles, tendons, or bone. In addition, the total body surface area, or TBSA, affected by the burn also contributes to the severity, since burns that involve over 10% are more likely to cause systemic complications.
Now, there are various complications associated with burn injuries, including infections, and fluid shifts, which can lead to dehydration and electrolyte imbalance. Burns also increase capillary permeability, causing a tremendous amount of fluid to shift from the plasma to the interstitial space, which is called “third-spacing”. As a result, intravascular volume is decreased, which decreases venous return to the heart, and ultimately cardiac output. Ultimately, this may lead to hypovolemic shock, where there’s inadequate organ perfusion of vital organs that leads to tissue hypoxia and cellular damage. When blood flow to the kidneys decrease, there can be acute kidney injury, which is one of the main causes of death for clients with burn injury. When the brain undergoes ischemia, there can be altered mental status. Ischemia of the gastric mucosa can lead to the development of a type of gastric stress ulcer, called Curling ulcer. Without the protection of the skin, the body is also at a higher risk for infections and sepsis, which can lead to septic shock weeks after the initial injury.
Another complication of burns is an alteration in thermoregulation, since a lot of heat is lost from the burned area. The risk of venous thromboembolism, such as deep venous thrombosis or pulmonary embolism, is also increased, mainly due to the damage to the vessel walls, and the prolonged period of bed rest. Finally, the body's response to the burn involves releasing more stress hormones, which results in a hypermetabolic state, and increased demand for glucose.
Now, electrical burns often affect the cardiac muscle and can lead to the development of arrhythmias. Electrical burns and burns that damage skeletal muscle tissue may cause rhabdomyolysis, or breakdown of skeletal muscle fibers, which releases myoglobin into the circulation. Myoglobin is toxic to the renal tubular epithelial cells, causing acute tubular necrosis, which can lead to acute renal failure.
In addition, certain burn locations are at a higher risk for the development of specific complications. For example, circumferential burns of the neck, or chest burn injuries can compress the trachea or impair breathing mechanics, leading to pulmonary complications. Also, if the burn is near the eye, it may cause corneal abrasion, which is a scratch on the superficial layer of the eye. If the injury is near the ear, it may cause auricular chondritis, which is inflammation of the ear cartilages. Burns of the perineal area may also be contaminated by urine or feces, leading to inflammation of the perineum.
Finally, depending on the cause of the burn, other complications may include carbon monoxide poisoning, and smoke inhalation injury, where the respiratory tract is damaged by breathing in smoke or harmful gasses.
Okay, now the clinical manifestations of a burn injury depend on the degree of the burn. In first-degree burns, the affected area becomes red, dry, and painful. These areas also tend to blanch, turning white as blood flow is restricted with compression. Second-degree superficial partial thickness burns can be red with clear blisters; wet, as if they are weeping; and are even more painful than first-degree burns. A second-degree deep partial thickness burn may vary in color from yellow or white to red; have blisters, and can be wet or dry. Because of damage to blood vessels and nerve endings, burns of this degree may only be painful due to pressure. Now, in a third-degree burn, an eschar starts to appear, which describes dead cells that fall off the skin, causing it to look waxy white to leathery gray or black; and dry, with edema underneath it. Again, blanching doesn’t occur and they can be painless due to extensive nerve damage, and may only feel deep pressure. Additionally, the elastin damage causes the burn to be stiff or inelastic. Finally, fourth-degree burns are charred black; dry and are totally painless due to the complete destruction of nerve endings. Having said that, the margins of all burns often have lots of damaged nerve endings and that can be painful.
The diagnosis of a burn injury starts with the client’s history and physical assessment, sometimes followed by tissue biopsies, which are obtained to accurately determine which layers are affected. In adults, the severity of burns is calculated using the rule of nines. The rule of nines evaluates several distinct sections of the body’s total surface area for the presence and degree of burns. Eleven of the sections each make up 9% of the body’s surface area and are: the head; right arm; left arm; chest; abdomen; upper back; lower back; the front of the left leg; and the back of the left leg; and the same for the right leg. A final section, the groin, accounts for the missing 1% of the body’s surface area.
So, once diagnosis of a burn is confirmed, laboratory tests are typically performed to rule out complications. These tests include a complete blood count and an electrolyte panel, along with hemoglobin and myoglobin levels in the urine. Finally, in cases of inhalational injuries or carbon monoxide poisoning, arterial blood gases and carboxyhemoglobin levels should be measured.
The treatment for a burn injury is determined by what caused the burn, the rule of nines, and the locations of the burns on the body. In general, immediate treatment typically includes removing the client from the source, removing all clothing, and preventing further burning; like flushing the burn with cool, but not ice-cold, running water. Maintaining airway, breathing, and circulation is also a priority. So, continuous airway assessment, as well as supplemental oxygen administration, are important.
After all this, it’s crucial to manage pain with medication.
Minor burns, like first- and second-degree superficial thickness burns, can heal on their own over a few days or weeks if kept bandaged, and clean with soap and water. Sometimes lotions to prevent drying or topical antibiotics can be used. If blisters form, it’s best to leave them alone because the intact skin helps prevent infections.
Now, hospitalization in specialized burn centers is often needed for more serious burns, like partial thickness burns that cover more than 10 percent of the total body surface area; burns in sensitive areas like the face, hands, feet, genitalia, perineum, or major joints; third degree burns; as well as electrical and chemical burns. In addition, clients with serious associated trauma or preexisting medical disorders, children with burns in unequipped hospitals, and those requiring special social, or emotional intervention should be transferred to specialized burn centers.