COVID-19: Nursing
COVID-19: Nursing
Respiratory
Respiratory
Notes
| COVID-19 | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
COVID-19 is a highly contagious disease that predominantly affects the respiratory tract. This disease is caused by the SARS-CoV-2 virus, which is a type of coronavirus. It’s a single-stranded RNA virus with a crown of protein spikes that stick out on the outer surface. The name can be broken down as follows: SARS is for severe acute respiratory syndrome; CO is for corona, VI is for virus, D is for disease, and 19 is for 2019, the year it was first identified.
Now, let’s quickly review the respiratory tract, which can be divided into two regions: the upper respiratory tract and lower respiratory tract. The upper respiratory tract includes the nose, nasal cavity, the oral cavity, pharynx, epiglottis, larynx, and the upper part of the trachea; while the lower respiratory tract includes the lower part of trachea, and the lungs containing the bronchi, bronchioles, alveolar ducts, and finally the alveoli.
Alveoli are tiny air-filled sacs where most gas exchange occurs, so as we breathe, the inhaled oxygen moves from the alveolar sacs into the blood, while the carbon dioxide moves from the blood into the alveolar sacs to be exhaled.
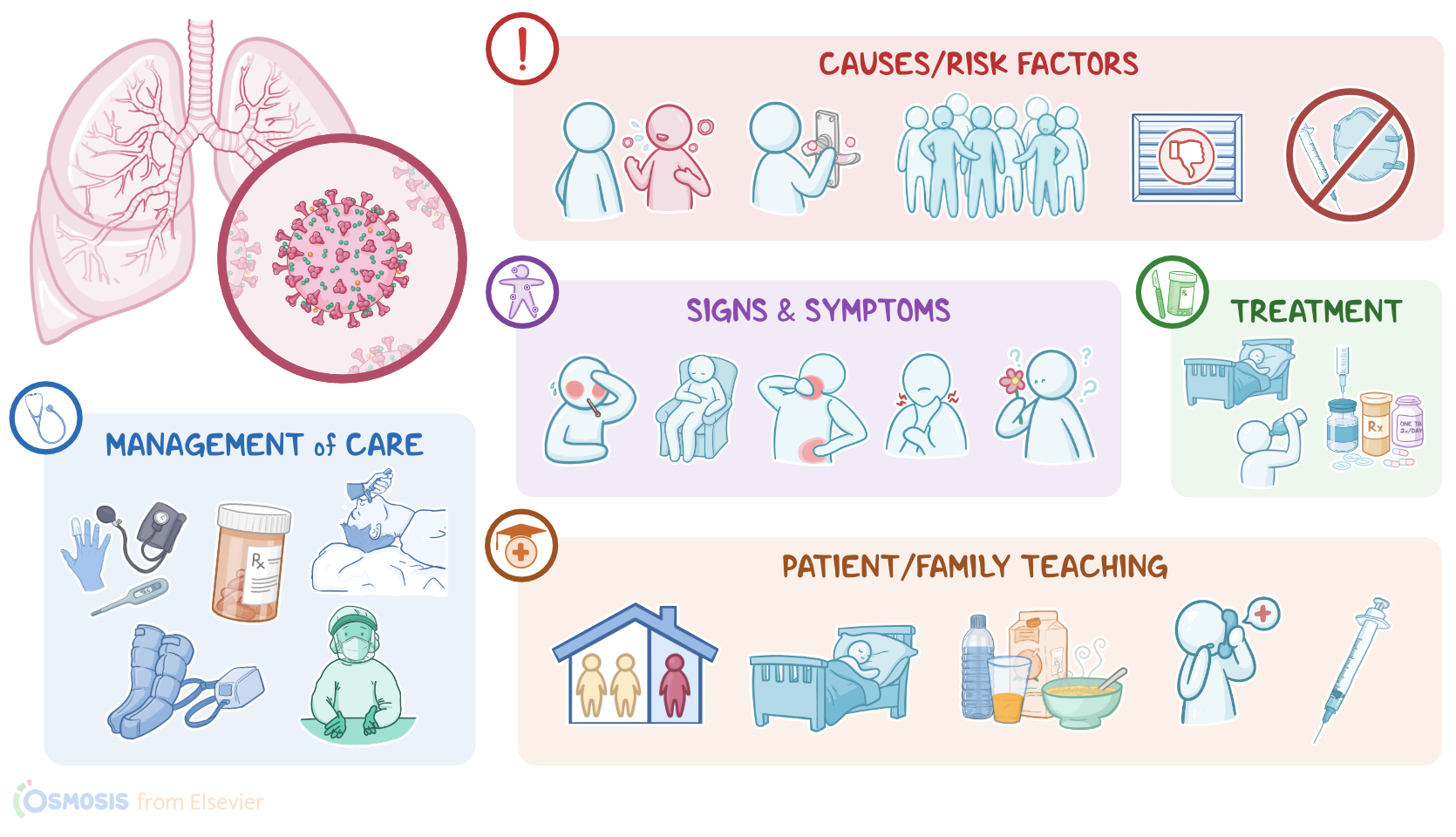
Okay, so COVID-19 is caused by the SARS-CoV-2 virus entering the respiratory tract. The virus is most often spread from person to person through tiny, aerosolized particles and larger droplets, which are expelled when an infected individual talks, sneezes, or coughs. The droplets can ultimately reach the respiratory tract of another person when they’re inhaled, or land on their eyes, nose, or mouth. Since the droplets don’t travel far, they tend to settle on surfaces, so, less frequently, the virus can be transmitted indirectly when an individual touches a contaminated surface and then, prior to washing their hands, they touch their eyes, nose, or mouth.
On the other hand, aerosolized particles can remain suspended in the air for longer periods and travel further distances, so they can cause infection when they’re inhaled.
Risk factors for getting COVID-19 include older age; pregnancy; having underlying health conditions, such as chronic lung disease, cancer, or diabetes mellitus; being immunocompromised; and not being fully vaccinated. The risk of infection also increases when in close contact with infected individuals, particularly in poorly ventilated indoor spaces or crowded settings. Infected individuals are most likely to spread the virus 1 to 2 days before symptom onset until about 10 days after symptom onset.
The virus typically enters the body through the nose or mouth. Once inside the body, the viral spikes on the SARS-CoV-2 virus bind to a protein called angiotensin-converting enzyme-2 or ACE2 for short, which is found mainly on host cells like respiratory epithelial cells and pneumocytes. Pneumonocytes make up the alveoli, where gas exchange occurs. It can also invade cells in the intestine, heart, blood vessels, kidneys, and bladder. The viral invasion and replication initiate an inflammatory response which damages the alveoli, as well as any other tissue infected.
Depending on the severity of alveolar damage, symptoms may vary. Some clients with COVID-19 can be asymptomatic. When present, the most common symptoms include fever, chills, fatigue, myalgia, headaches, a new loss of taste or smell, sore throat, cough, and dyspnea, as well as nausea, vomiting, diarrhea, or abdominal pain.
Less commonly, clients may present with conjunctivitis, skin rashes, and confusion or delirium.
In the most severe cases, complications may develop, like acute respiratory distress syndrome, as well as cardiovascular or thromboembolic events, sepsis, and acute kidney injury.
Now, diagnosis of COVID-19 begins with a history considering possible exposure, signs and symptoms, and physical assessment; followed by viral tests to confirm the diagnosis. There are two types of viral tests: nucleic acid amplification tests like RT-PCR, which detects viral RNA; and antigen testing, which detects viral antigens such as those found on the spike, or S, protein. Clients may receive tests from a healthcare provider or perform self-tests using an at-home testing kit.
Additional tests can be performed to determine the severity of the disease. Laboratory tests may show normal or decreased white blood cells; elevated CRP, indicating inflammation; and increased liver function tests like LDH, AST, ALT. Severe cases may show abnormal coagulation tests like an increased PT, INR, and D-dimer. In addition, chest X-rays or CT scans can be performed to assess disease severity or complications.
Finally, if there is a need to determine whether a client has previously had a COVID-19 infection, or to assess their immune response to the virus, clients who previously had known or suspected COVID-19 may get serologic tests to detect antibodies against SARS-CoV-2.
There’s no cure for COVID-19, so treatment involves supportive therapy to reduce the symptoms and antiviral medications when needed. Supportive care includes rest and hydration, as well as medications like analgesics, antipyretics, and antihistamines. Antiviral medications work by slowing down or stopping replication of the virus, reducing the amount of virus in the body.
Mild cases are typically treated at home; while some moderate cases may warrant hospitalization for close monitoring, as well as supplemental oxygen as needed. Severe cases require hospitalization, supplemental oxygen, and medications like glucocorticoids, antivirals, and thromboprophylaxis, as well as management of complications. Finally, the most effective way to prevent COVID-19 is through vaccination.
Alright, now let's look at the nursing care you’ll provide for a client with COVID-19. The priority goals of your nursing care are to improve your client’s respiration and oxygenation; to prevent and manage systemic complications; and to prevent the spread of the disease.
Begin by assessing your client’s respiratory status, breath sounds, and oxygen saturation. Keep their SpO2 between 92% and 96% by administering high-flow oxygen, as ordered.
If they develop shortness of breath and their SpO2 is consistently below 92%; report your findings to the healthcare provider and implement the prescribed interventions, including non-invasive positive-pressure ventilation and prone positioning.
Continue to closely monitor their vital signs, SpO2, and arterial blood gases, or ABGs; report the development of severe acidosis and worsening hypoxemia; and prepare for intubation and mechanical ventilation. Lastly, administer glucocorticoids and antiviral medications as ordered.
Then, be sure to monitor your client for signs and symptoms of cardiovascular and hematological complications of COVID-19. Review their baseline diagnostic tests, such as ECG, BNP and troponin levels, and report ECG changes, or a rise in BNP and troponin, which could indicate myocardial injury. Also, keep a close eye on their coagulation studies; and promptly report indications of disseminated intravascular coagulation, including thrombocytopenia, increased D-dimer, increased fibrin degradation products, and prolonged PT.
Be prepared to provide supportive care and administer blood products as ordered. Also, promptly report if you notice signs of unusual clotting, such as microvascular thrombosis of the toes, sometimes called COVID toes, which can manifest as swelling, usually with a pinkish or reddish discoloration on lighter skin tones, or a purplish hue in darker skin tones. In addition, be sure to report any clotting of intravascular catheters; as well as any signs of deep vein thrombosis, such as warmth, swelling, and reddened or darkened skin around a painful area in a lower extremity;
clinical manifestations of pulmonary embolism like anxiety, a sudden onset of dyspnea, or a client report of chest pain; and any signs and symptoms of stroke, which could manifest as facial drooping, difficulty speaking, or a sudden and severe headache, dizziness, and confusion.
Sources
- "Lewis’s Medical-Surgical Nursing: Assessment and Management of Clinical Problems. 12th Edition. ISBN:978-0-323-78961-5 " Elsevier (2023)
- "McCance & Huether’s pathophysiology: The biological basis for disease in adults and children (9th ed.). ISBN: 978-0-323-78987-5 " Elsevier (2023)