Cirrhosis: Nursing process (ADPIE)
2,566views
Cirrhosis: Nursing process (ADPIE)
Synthesis Of Nursing Practice
Synthesis Of Nursing Practice
Notes
| CIRRHOSIS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Contributors
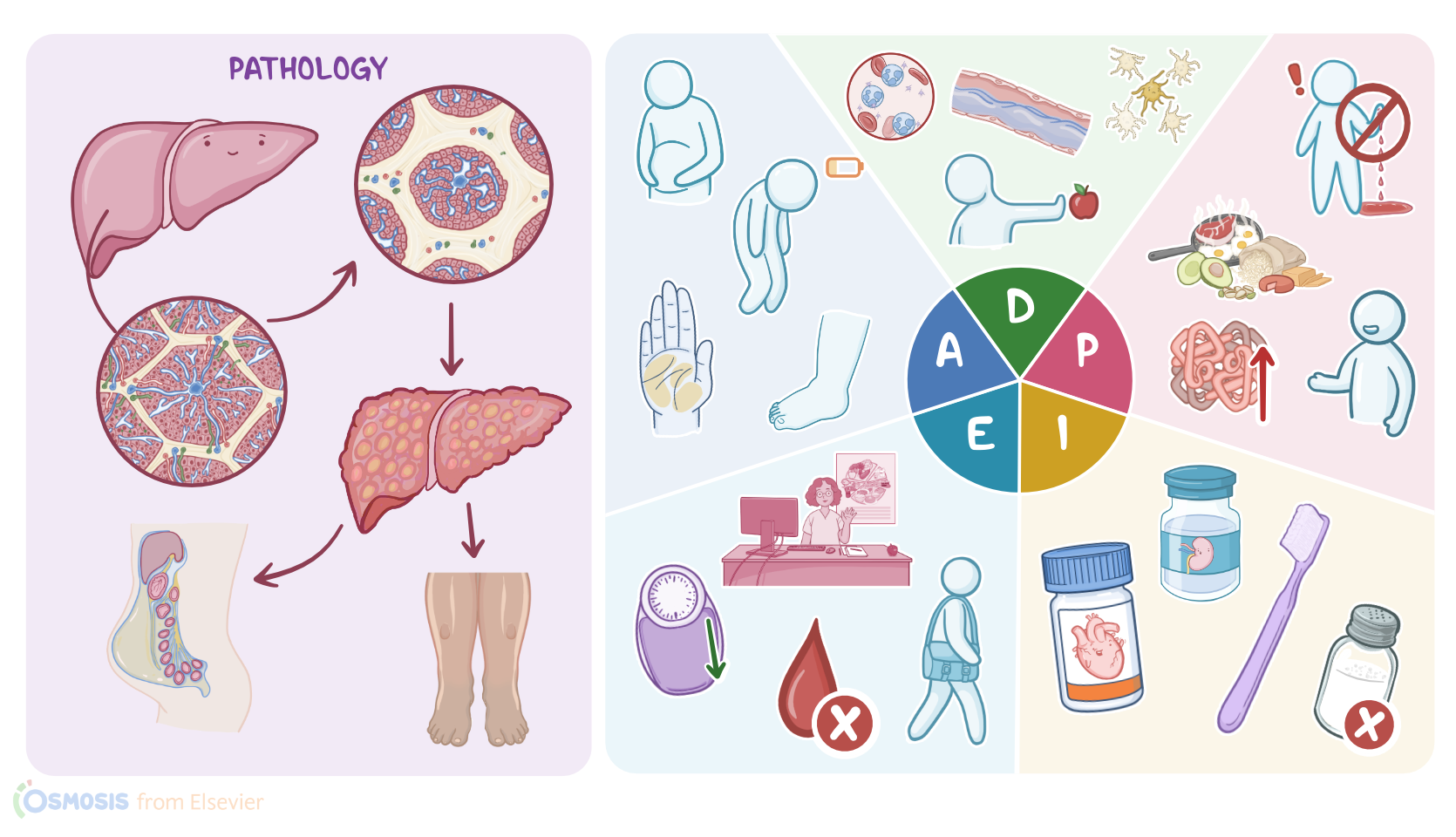
Rita Davis is a 55-year-old African American woman with a history of cirrhosis from chronic hepatitis C infection.
Today, Rita is visiting the clinic for concerns about increased abdominal distention, loss of appetite, and fatigue.
Cirrhosis is a condition in which the liver, a large organ in the right upper quadrant of the abdomen, becomes irreversibly scarred from chronic inflammation.
Because the liver has many functions related to digestion, metabolism, detoxification, and production of important molecules the body needs, damage to the liver can have widespread impact on a person’s health.
Let’s look at some of the contributing factors for chronic liver inflammation.
One of the most common modifiable risk factors is long-term alcohol use.
On the other hand, non-modifiable risk factors for cirrhosis include viral hepatitis, autoimmune hepatitis, and other autoimmune disorders, including primary biliary cholangitis and primary sclerosing cholangitis, which can cause liver injury through progressive scarring of the bile ducts.
Liver injury can also occur from non-alcoholic fatty liver disease, in which fat cells build up in the liver.
Genetic disorders like hemochromatosis and Wilson’s disease can cause inflammation from accumulating elements like iron or copper in the liver, whereas alpha-1 antitrypsin deficiency creates malformed proteins that become stuck in the liver.
The liver is highly regenerative, meaning that after injury it replaces injured tissue with regenerative nodules.
These nodules are colonies of liver cells, or hepatocytes, surrounded by collagen-rich scar tissue.
This causes the smooth liver tissue to become bumpy and stiff.
Over time, inflammation causes bands of scar tissue to form between nodules.
As the scar tissue grows, it compresses the network of blood supply in the liver.
This leads to increased venous pressure and portal hypertension, which occurs as blood backs up into the portal vein.
Now, higher portal vein pressure means that fluid in blood vessels is more likely to get pushed into tissues, leading to peripheral edema, as well as into large open spaces, like the peritoneal cavity, which is known as ascites.
To make matters worse, damage to the liver impairs its ability to make albumin, which is a protein in blood that helps keep fluid within the blood vessels.
Hypoalbuminemia, or low albumin in the blood, contributes to ascites as well as peripheral edema.
Ascites typically presents as a distended abdomen, which can be detected by the presence of a fluid wave that means there is free fluid in the abdomen; as well as shifting dullness, which presents as a change during percussion from tympany, where fluid is, to dullness when the fluid moves as the client’s position is changed.
Unfortunately, ascites fluid can become infected without an obvious cause, called spontaneous bacterial peritonitis.
Signs of this complication include fever, abdominal pain and tenderness, nausea, vomiting, and altered mental status.
The increased venous pressure within the gastrointestinal tract ultimately leads to dilation of the gastrointestinal veins, which become fragile, and are called varicose veins, or varices.
The veins can often be seen as radiating out from the umbilicus, a condition called caput medusae.
On the other hand, varices in the esophagus or stomach are the most prone to rupture and bleeding, which can be a life-threatening complication.
Signs of variceal bleeding include hematemesis, melena, hypotension, and tachycardia.
As pressure in the portal system builds, the spleen can become distended, causing splenomegaly.
The enlarged spleen traps red blood cells, leading to anemia, and white blood cells, causing leukopenia and increasing the risk of infection.
Also platelets become trapped within the spleen, causing thrombocytopenia, resulting in easy bruising or bleeding.
Bleeding and bruising are also a result of the liver not being able to synthesize clotting factors, like prothrombin.
When the blood takes longer to clot, PTT, PT, and INR levels may be increased.
Over time, the declining liver function means that toxins and waste products don’t get metabolized.
Elevated levels of bilirubin circulating in the body causes jaundice and pruritus.
Ammonia and other toxins can build up in the brain leading to hepatic encephalopathy.
This neurological complication of liver disease causes a flapping tremor, called asterixis, as well as changes in mental status or behavior, and can ultimately lead to coma.
Impaired liver function means that hormones like estrogen don’t get metabolized, so their levels increase, leading to the development palmar erythema.
In males, testicular atrophy, gynecomastia, and loss of sex drive can be present.
On the other hand, premenopausal females may experience an absence of menstruation, while older females may experience vaginal bleeding.
Finally, impaired metabolism by the liver of vitamin D can cause loss of bone density and osteoporosis.
Diagnosing cirrhosis involves analyzing blood work, which most commonly shows increasing serum levels of ALT, AST, ALP, or GGT, as these liver enzymes leak into the bloodstream from damaged liver cells.
Liver nodules associated with hepatic injury may be seen on ultrasound, CT scan, or MRI.
Magnetic resonance elastography uses an MRI along with low-frequency vibrations to assess for stiffening of the liver.
Finally, a liver biopsy can be done to confirm the stage or exact cause of cirrhosis.
Treatment of cirrhosis involves preventing further liver damage by addressing the underlying cause.
Lifestyle changes include avoiding alcohol and hepatotoxic medications, such as acetaminophen, as well as eating a healthy low-sodium diet, and preventing infections with good hand hygiene and avoiding people who are sick.
Antihypertensives like beta-blockers are used to reduce portal hypertension.