Erysipelas and cellulitis: Nursing
1,605views
Erysipelas and cellulitis: Nursing
2144 final exam
2144 final exam
Notes
| ERYSIPELAS AND CELLULITIS | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
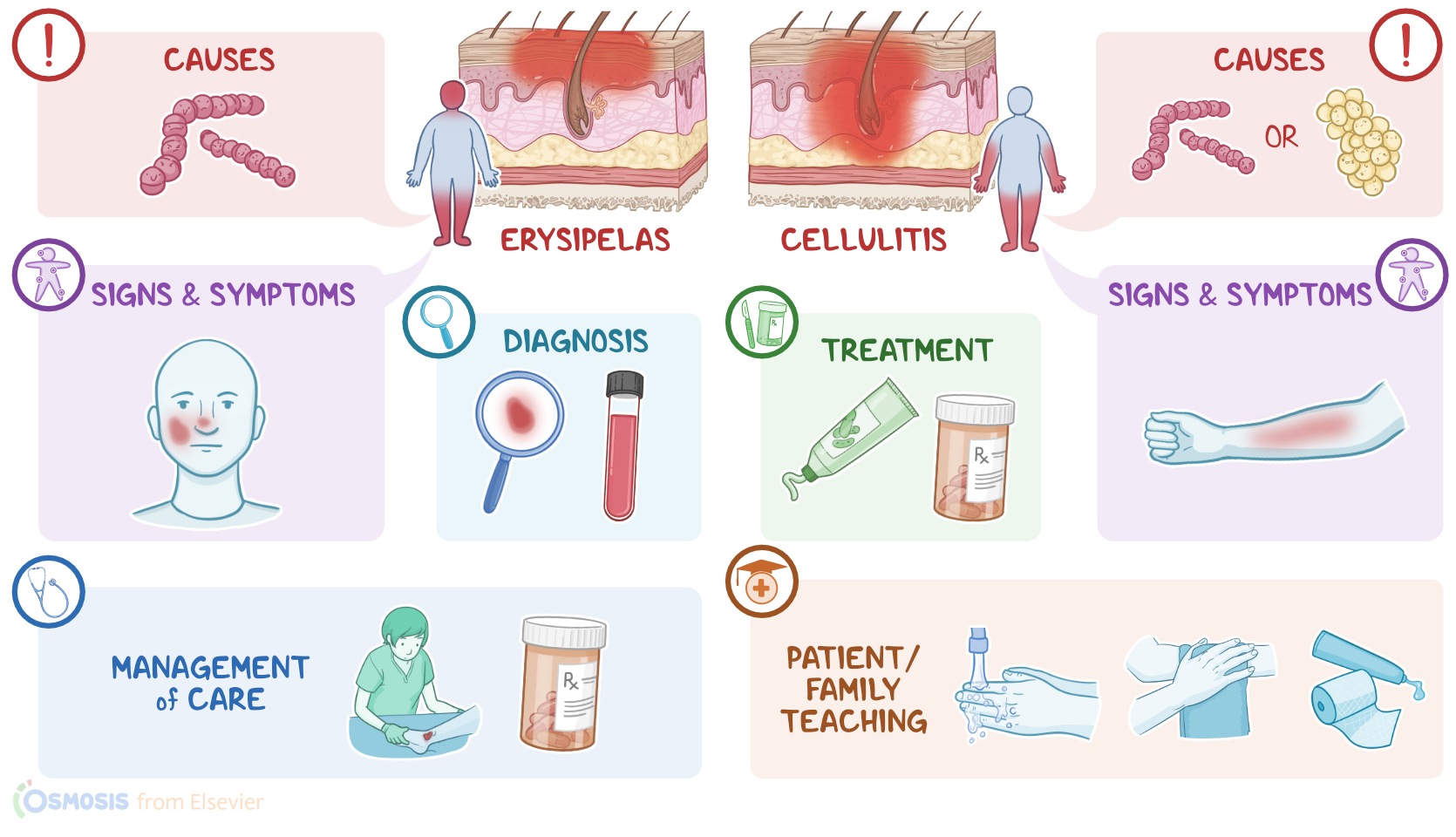
Erysipelas is a superficial bacterial skin infection that involves the upper dermis, whereas cellulitis is a deeper bacterial skin infection involving the deeper dermis and subcutaneous tissues.
Okay, let’s go over some physiology. Normally, the skin is divided into three layers, the epidermis, dermis, and hypodermis. The hypodermis is made of fat and connective tissue that anchors the skin to the underlying muscle. Just above the hypodermis is the dermis, which contains hair follicles, nerve endings, glands, blood vessels, and lymphatics. And just above the dermis is the epidermis, which itself has multiple cell layers that form the external skin surface.
Now, normally, the skin surface is colonized by a huge number of microorganisms that make up the normal skin flora. This flora consists mostly of bacteria, such as Staphylococcus epidermidis, as well as certain fungi, such as Candida albicans. The normal skin flora is typically non-pathogenic, meaning that these microorganisms don’t cause any disease. In fact, they are beneficial, since they serve as a physical and competitive barrier that helps prevent pathogenic microorganisms from invading and infecting the skin.
Now, both erysipelas and cellulitis are typically caused by Gram positive pathogenic bacteria. For erysipelas, the most common causative bacterium is Streptococcus pyogenes, also called group A β-hemolytic Streptococcus; whereas cellulitis is usually caused by Streptococcus pyogenes or Staphylococcus aureus.
Risk factors that can allow these bacteria to invade the skin include having previous damage due to insect bites, minor trauma, abrasions, or skin conditions like eczema, as well as previous skin infections like impetigo or a history of cellulitis.
Additional risk factors include older age, obesity, diabetes mellitus, arteriovenous insufficiency, lymphatic obstruction, and immunocompromised clients. Now, erysipelas occurs when pathogenic bacteria find a way to invade the skin and cause infection of the upper dermis, and may often extend to the superficial lymphatic vessels of the underlying connective tissue. On the other hand, cellulitis occurs when bacteria manage to affect the deeper dermis and subcutaneous tissues.
In severe cases, these infections may cause complications, such as the formation of abscesses, as well as extensive tissue damage and necrosis, which can result in gangrene. Another complication is necrotizing fasciitis, where the infection involves the subcutaneous tissues and fascia. If the infection keeps spreading to underlying tissues like bone, it can result in osteomyelitis. Lastly, if the infection spreads to the blood, it may result in sepsis.
Okay, moving onto clinical manifestations. Erysipelas means “red skin” in Greek and most commonly involves the face or the lower limbs. It typically presents as a red, swollen, and tender skin area that might be warm to the touch. The lesions are sharply defined and well-demarcated, with slightly elevated borders and reddish streaks of lymphangitis. In more severe cases, there can also be vesicles or bullae.
On the other hand, cellulitis commonly manifests in the limbs. Typically presents as a red, swollen, and tender skin area that’s warm to the touch. But unlike erysipelas, the infectious process in cellulitis is deep underneath the skin, so the lesions are poorly demarcated and have hardly noticeable margins.
Finally, some clients with erysipelas or cellulitis may also present with fever, chills, and lymphadenopathy.
Now, the diagnosis of erysipelas and cellulitis primarily involves the client’s history and physical assessment. There are no specific laboratory tests, but a complete blood count may reveal leukocytosis, as well as increased inflammatory markers like ESR and CRP.
Treatment of erysipelas and cellulitis is chosen based on the severity of the infection, as well as the efficacy and response to treatment. For mild cases, treatment is administered topically and includes warm compresses, rest, elevation of the affected limb, antibiotic dressings and ointments.
In more severe cases, clients can be treated with systemic antibiotics, such as penicillin, or more rarely, clients may need hospitalization and administration of intravenous antibiotics, such as vancomycin, linezolid, and ceftaroline.