Esophageal cancer: Nursing
Esophageal cancer: Nursing
M1 April: Foundations of Oncology
M1 April: Foundations of Oncology
Notes
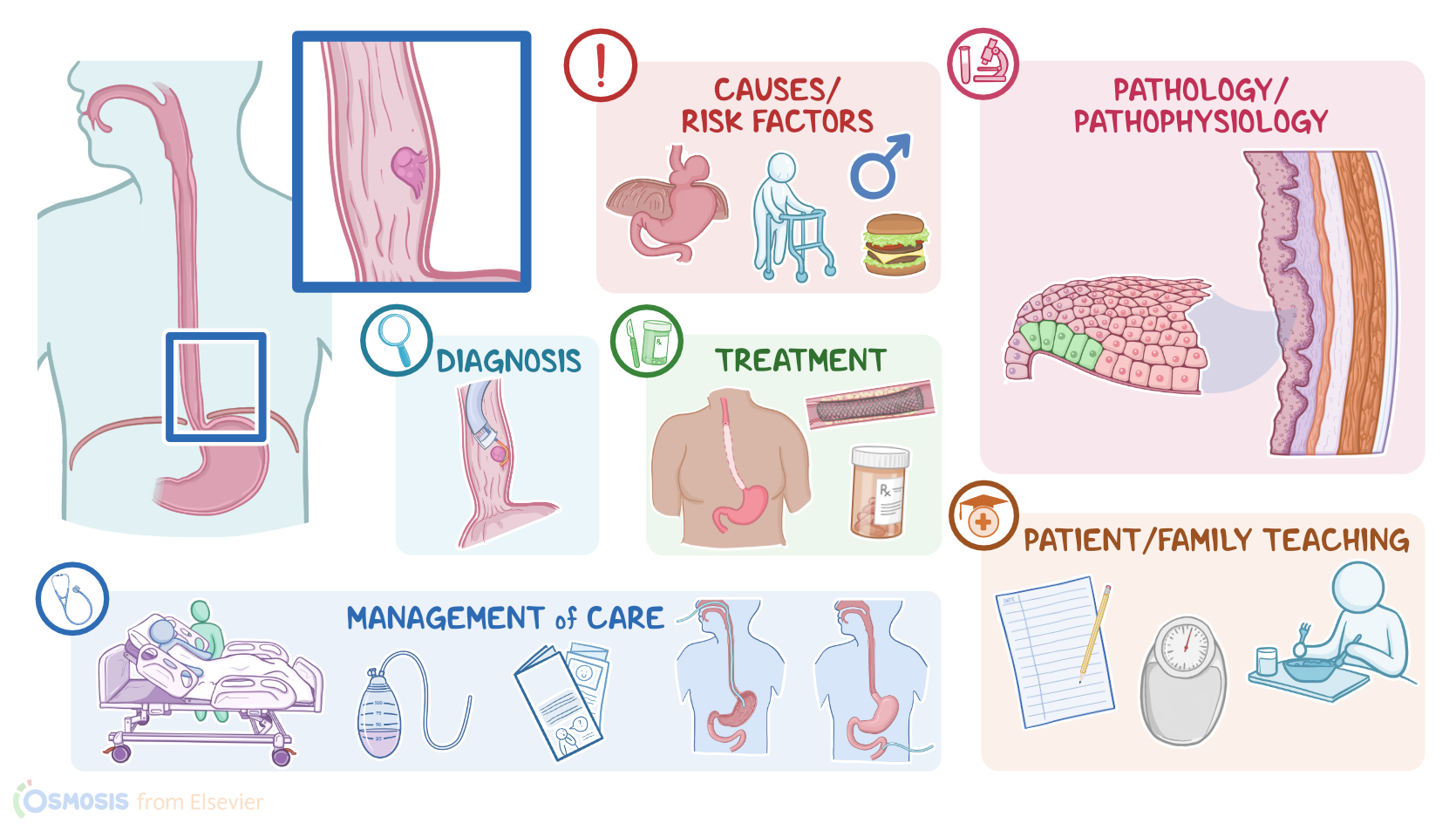
| ESOPHAGEAL CANCER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Esophageal cancer is a malignant tumor that originates in the mucosa of the esophagus. There are two types of esophageal cancer, squamous cell carcinomas and adenocarcinomas.
Alright, now, the esophagus is a hollow tube that allows food to pass through from the pharynx to the stomach. And at both ends is a sphincter or a bundle of muscles that can block off or open the esophagus. The upper esophageal sphincter relaxes to allow food to pass through. The lower esophageal sphincter contracts to prevent acid reflux from the stomach.
Let’s zoom into the wall of the esophagus, which is made up of four layers. The outermost layer is a fibrous layer called the adventitia, and unlike the rest of the gastrointestinal tract, this layer does not contain a serosa. Next is the muscular layer, which contracts to move food through the esophagus. After that is the submucosa, which consists of a dense layer of tissue that contains blood vessels, lymphatics, and nerves. And then, there’s the innermost layer, called the mucosa, which comes into direct contact with food, and protects the esophageal wall from friction. The mucosa also has three layers of its own: a layer made of stratified squamous epithelium; a layer of connective tissue called the lamina propria, and a layer of muscle cells called the muscularis mucosae. Finally, at the lower esophageal sphincter, the esophageal mucosa joins the columnar gastric epithelium to form the gastroesophageal junction.
Alright, now, esophageal cancer occurs when epithelial cells in the mucosa acquire mutations that let them grow and divide out of control. Typically these are mutations in proto-oncogenes which result in a promotion of cell division, or mutations in tumor suppressor genes which result in a loss of inhibition of cell division.
Now, mutations may arise due to a variety of risk factors. Risk factors for both squamous cell carcinoma and adenocarcinoma include age over 60 years, being assigned male at birth, asbestos exposure, and a diet high in pickled and fermented foods, red meat, fat, and processed foods; and low in fruit, and vegetables. Other risk factors include hiatal hernia, which is when part of the stomach bulges up into the chest through an opening in the diaphragm, and esophageal webs, or rings, which are concentric extensions of the normal esophageal wall into the esophageal lumen that can cause difficulty swallowing.
Specific risk factors for squamous cell carcinoma include smoking, excessive alcohol intake, excessive intake of very hot fluids, and caustic strictures, which is the narrowing of the esophagus following ingestion of a caustic substance, like household bleach. Another predisposing condition is achalasia, which is when the smooth muscle of the lower portion of the esophagus doesn’t work well, making it difficult for food to pass towards the stomach.
On the other hand, the strongest risk factor for adenocarcinoma is obesity, and gastroesophageal reflux disease, or GERD for short. That’s because, with GERD, the lower esophageal sphincter is weaker than normal, and it allows acid from the stomach to go back up into the esophagus after meals. The chronic presence of acid in the esophagus can lead to Barrett’s esophagus, where the distal part of the esophagus undergoes intestinal metaplasia. This is where the normal squamous epithelium in the esophagus tries to adapt to the increased acidity by turning into columnar glandular epithelium that’s normally found in the intestine.
Moving on to pathology, a squamous cell carcinoma develops when the mutated cells originate in the squamous epithelium, typically in the proximal two-thirds of the esophagus. In contrast, adenocarcinomas develop when the mutation occurs in the glandular epithelium, typically in the distal third of the esophagus.
Alright, now once an epithelial cell becomes mutated and cancerous, it starts dividing uncontrollably, forming a tumor mass. As the tumor keeps growing, new blood vessels also develop via angiogenesis to supply it. Eventually, cancerous cells start invading neighboring tissues, such as the trachea and the diaphragm. This spread can be aggressive because the esophagus is not surrounded by a serosal layer.
Esophageal cancer may also spread to nearby lymph nodes, or may metastasize to distant organs, such as the liver and lungs.
Complications of esophageal cancer include esophageal obstruction, hemorrhage, perforation, and tracheoesophageal fistula formation, which is an abnormal connection between the trachea, and the esophagus.
Now, the clinical manifestations of esophageal cancer vary based on the size and location of the tumor. Initially, clients can be completely asymptomatic. Over time, the body mounts an immune response to fight the tumor off, so clients may start experiencing unintentional weight loss, fever, and malaise.
If the tumor grows enough to physically obstruct the esophageal lumen, it can cause dysphagia or progressively difficult swallowing. At first, dysphagia is specific to solid foods, but as the disease progresses, liquids are also hard to swallow. Other symptoms include odynophagia, or pain when swallowing, heartburn, pain in the chest or back, and halitosis, or bad breath. If the tumor surface bleeds, clients may also present with vomiting of blood, and iron deficiency anemia. If a tracheoesophageal fistula is present, it may lead to pulmonary aspiration of esophageal contents, which may cause symptoms like coughing and dyspnea. Finally, if esophageal cancer spreads to the diaphragm, it can cause hiccups.
Diagnosis of esophageal cancer starts with the client’s history and physical assessment, followed by endOscopy with biopsy. Additional imaging via a CT, PET scan, or endoscopic ultrasound can be used to determine the stage of the tumor in the TNM system, where T stands for tumor location and local spread; N stands for lymph node involvement; and M for whether or not the tumor has metastasized.