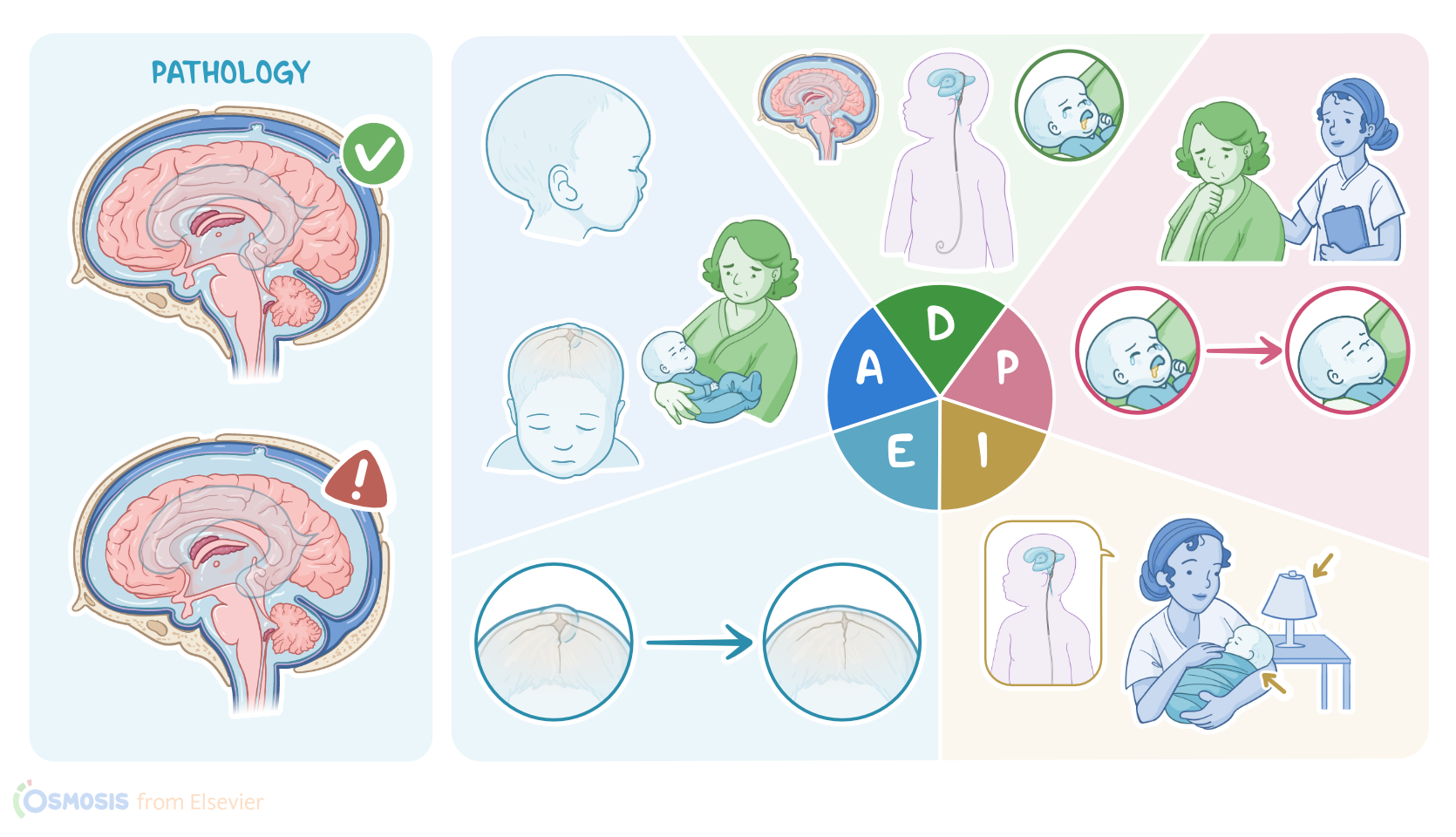
Hydrocephalus: Nursing process (ADPIE)
Notes
| HYDROCEPHALUS | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
Ishaan Mondal is a 5 week old male who presents with an increased head circumference, vomiting, and irritability. His mother, Ziva, reports that while Ishaan appears hungry, he has difficulty suckling when attempting to breastfeed. After an appointment with his pediatrician, Ishaan is directly admitted to the neonatal intensive care unit, or NICU, for monitoring and treatment of hydrocephalus.
Hydrocephalus refers to the excessive buildup of cerebrospinal fluid, or CSF, within the brain. The CSF helps provide cushion and protection, as well as metabolic fuel for the brain. Now, the brain has two lateral ventricles, as well as the third and fourth ventricles, which are all interconnected, and each one contains a structure called a choroid plexus. The choroid plexus is made up of ependymal cells, which produce the CSF that can drain down to the fourth ventricle. From there, the CSF enters the subarachnoid space, and gets reabsorbed by arachnoid granulations into the dural venous sinuses, which are pools of venous blood. Finally, the CSF and venous blood are drained together out of the skull and into the internal jugular vein. Now, since the skull is such a rigid structure, the volume of the brain, CSF, and blood must be constant and in balance. So, with hydrocephalus, the increased CSF volume causes the four ventricles to enlarge and intracranial pressure to rise, which can compress and damage brain structures.
Now, there are two types of hydrocephalus. Noncommunicating, or obstructive hydrocephalus, is caused by an obstruction of the CSF flow anywhere along its path. This can be caused by a brain tumor, cyst, or by congenital causes, like cerebral aqueduct stenosis. On the other hand, communicating, or nonobstructive hydrocephalus is most often caused by decreased CSF reabsorption. This occurs when there’s inflammation or obstruction of the arachnoid granulations, which can be caused by infections, such as meningitis, as well as subarachnoid hemorrhage. Less frequently, communicating hydrocephalus can be caused by increased CSF production, like by a choroid plexus tumor.
Now, there are some factors that can put the client at increased risk of hydrocephalus. Non-modifiable risk factors include male sex, having a family history of hydrocephalus, and some congenital malformations affecting the CSF flow. On the other hand, modifiable risk factors include being unvaccinated against common bacteria that cause meningitis, as well as experiencing head trauma, which may lead to subarachnoid hemorrhage. Other possible modifiable risk factors include gestational diabetes mellitus, as well as the lack of prenatal care before pregnancy, which may increase the risk of congenital infections like congenital syphilis and rubella.
Now, the main symptoms of hydrocephalus result from the increased intracranial pressure and include headache, nausea, vomiting, as well as seizures. In addition, clients may have blurred vision, unsteady gait, and impaired consciousness, which, in severe cases, may progress to coma. In infants, additional symptoms can include irritability, high-pitched cry, and a downward deviation of the eyes, which is called sunset eyes, as well as macrocephaly, which is an increase in head circumference. Moreover, infants can have bulging fontanelles, which are the soft spots in the infant’s skull where the cranial bones have not fused yet.
Clients with hydrocephalus have a higher risk of developing long-term complications, such as permanent visual impairment, speech impairment, and learning difficulties affecting the client’s attention, thinking, and memory formation. In children, this results in poor school performance. Other potential complications include recurrent seizures, as well as physical disabilities, such as balance problems, poor motor coordination, and muscle weakness.
Diagnosis of hydrocephalus begins with history and clinical findings. In addition, fundoscopic examination may show papilledema, which is the swelling of the optic nerve. Next, in infants younger than 6 months of age, where fontanelles are still present, cranial ultrasonography is typically done to visualize the enlarged brain ventricles, while in older children and adults, MRI is preferred. Finally, other tests can be performed based on the suspected cause, such as a lumbar puncture for meningitis, or CT scan to rule out a subarachnoid hemorrhage.
Now, the main treatment of hydrocephalus focuses on draining the excess CSF from the brain to decrease the intracranial pressure. If hydrocephalus develops over a short period of time, the intracranial pressure should be decreased with a lumbar puncture or by surgically placing a temporary shunt, such as an external ventricular drain into the brain ventricles. This allows monitoring of the intracranial pressure while also draining the excess CSF into an external collection bag. In young infants, an anterior fontanelle ventricular tap can be done, where a needle is inserted through the anterior fontanel and into the ventricles, which allows the excess CSF to drip out. Now, if hydrocephalus persists, the client may need surgical placement of a permanent shunt, which drains the excess CSF from brain ventricles to somewhere else in the body where it can then be absorbed into the bloodstream. The most commonly used shunt is ventriculoperitoneal shunt, or VP shunt for short, which drains the CSF into the peritoneal cavity in the abdomen. Finally, keep in mind that clients with a shunt need to be followed up for complications like shunt obstruction, disconnection, and infection.
Sources
- "Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care, 13th edition" Mosby (2022)
- "Medical-Surgical Nursing: Concepts for Interprofessional Collaborative Care, 10th Edition" Elsevier (2020)
- "Harrison’s Principles of Internal Medicine, 21st edition" McGraw Hill / Medical (2022)
- "Anaesthetic management for hiatal hernia repair in a child with Bartter's syndrome: A case report" J Pak Med Assoc (2020)
- "Critical Care Nursing: Diagnosis and Management, 9th edition" Elsevier (2021)
- "Syndromic Hydrocephalus" Neurosurg Clin N Am (2022)