Hyperparathyroidism: Nursing
Hyperparathyroidism: Nursing
Endocrine system
Notes
| HYPERPARATHYROIDISM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
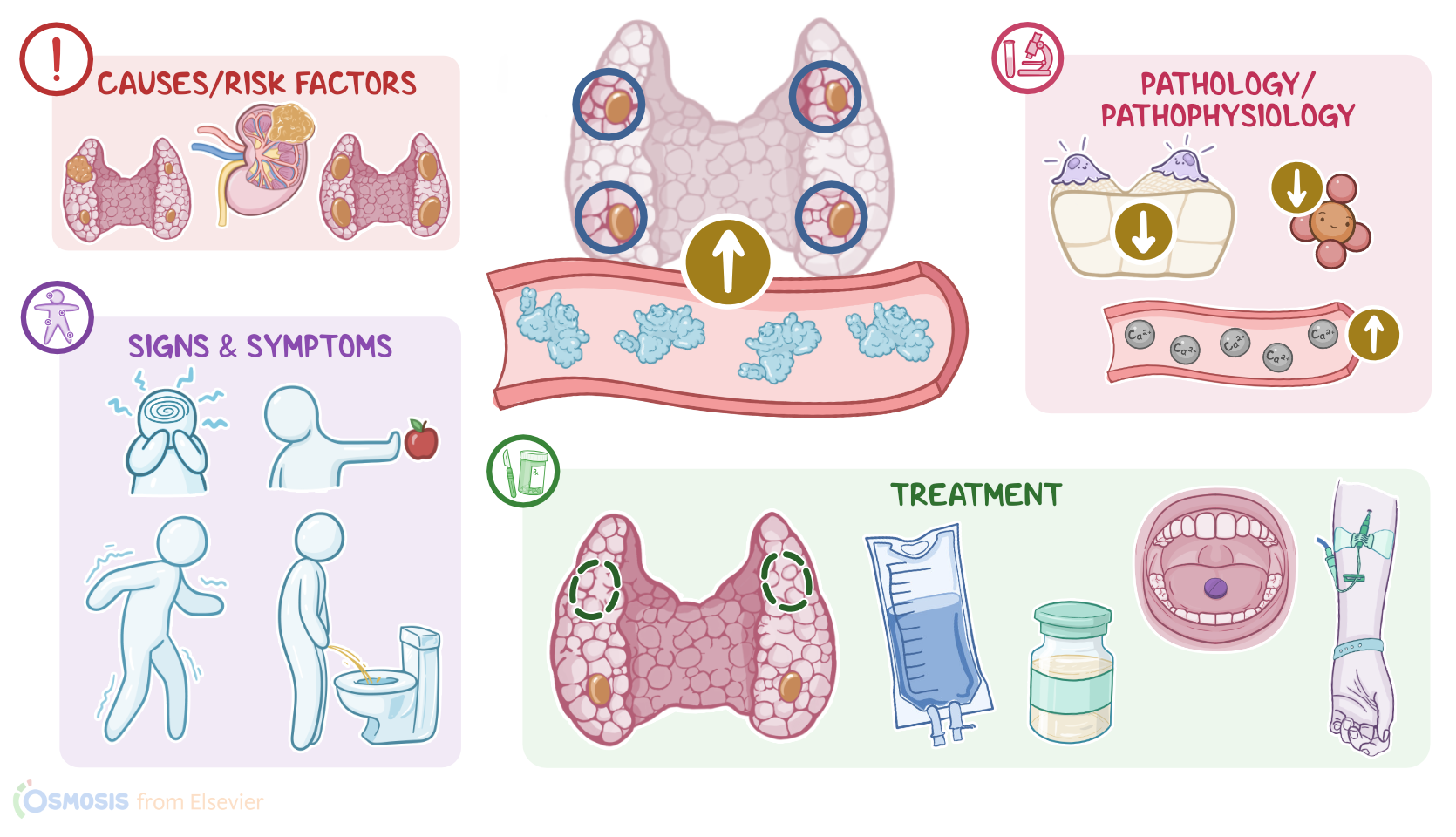
Hyperparathyroidism is a condition characterized by an increase in blood levels of the parathyroid hormone, or PTH for short, which ultimately results in hypercalcemia, or high blood calcium levels, as well as hypophosphatemia, or low blood phosphate levels.
Now, PTH is produced by four small glands called the parathyroid glands. These glands lie in the neck, being stuck to the back surface of the thyroid gland. The main function of PTH is keeping the levels of calcium within the normal range. For example, when calcium levels are low, PTH boosts bone resorption, which causes the release of calcium and phosphate from the bone into the bloodstream. In addition, PTH activates vitamin D, which in turn increases calcium and phosphate absorption from the gut. PTH also stimulates calcium reabsorption and phosphate excretion from the kidney. On the other hand, high calcium levels cause the secretion of PTH to fall, which increases the deposition of calcium in bones and the excretion of calcium by the kidneys.
Alright, now based on the underlying cause, hyperparathyroidism may be classified into three types. First is primary hyperparathyroidism, which is caused by congenital hyperplasia, parathyroid tumor or cancer, and neck radiation or trauma. Next is secondary hyperparathyroidism, which happens as a compensatory response to a condition outside the parathyroid glands that’s causing hypocalcemia, including vitamin D deficiency, chronic kidney disease, and PTH-secreting carcinomas of the lung and kidneys. Finally, there is tertiary hyperparathyroidism, which can happen in clients who had long standing secondary hyperparathyroidism, in which the parathyroids have been producing high levels of PTH for so long that they undergo hyperplasia, or enlargement, and stop responding to feedback from calcium levels in the blood. As a result, the parathyroids become permanently overactive, independently of blood calcium levels.
Now, risk factors of developing hyperparathyroidism include radiation therapy to the neck; nutritional deficiencies like calcium deficiency, or severe, ongoing vitamin D deficiency; being assigned female at birth; and lithium use.
Regardless of the underlying cause and type of hyperparathyroidism, excess PTH levels stimulate an increase in bone resorption, as well as a decrease in bone production, ultimately causing the bones to release calcium into the blood. In addition, there’s increased vitamin D activation, which in turn increases calcium absorption at the gut and calcium reabsorption from the kidneys. These changes add up to finally cause hypercalcemia, as well as hypophosphatemia.
Now, many organs and tissues throughout the body depend on normal calcium levels to function properly. This is especially important in the brain and the heart, where calcium inhibits neurons and cardiac pacemaker cells from depolarizing. As a result, hypercalcemia makes these cells less excitable.
Okay, so in clients with hyperparathyroidism, signs and symptoms are typically associated with hypercalcemia. These can include fatigue, and mental status changes, depression, confusion, and impaired memory; as well as loss of appetite, constipation, and muscle weakness, particularly in the proximal muscles of the lower limb.
Now, with hypercalcemia, the kidneys will need to work harder to filter the excess calcium, leading to hypercalciuria and polyuria, which can in turn cause dehydration. Also, the extra calcium circulating in blood may deposit in organs and tissues, leading to the formation of calcium based kidney stones and gallstones, as well as pancreatitis.
Hypercalcemia can also interfere with the electrical impulses that regulate the heartbeat, so clients may experience cardiac arrhythmias, as well as hypertension. Other complications of hyperparathyroidism include osteoporosis, which weakens the bones, rendering them prone to fractures.
The symptoms of hyperparathyroidism can be remembered as ‘stones, thrones, bones, groans, and psychiatric overtones’. ‘Stones’ is for calcium-based kidney stones or gallstones that can form. ‘Thrones’ refers to the toilet for polyuria. ‘Bones’ is for osteoporosis. ‘Groans’ is for constipation and muscle weakness. Finally, ‘psychiatric overtones’ refers to mental status changes.
The diagnosis of hyperparathyroidism starts with history and physical assessment, followed by laboratory tests. These tests include increased blood levels of PTH, as well as hypercalcemia, and hypophosphatemia; in addition to decreased urine levels of cyclic adenosine monophosphate, or cAMP for short, and hypercalciuria.
Abdominal X-rays can also be done to exclude kidney stones and calcium deposits, and to check for decreased bone density from osteoporosis and the presence of bone lesions from abnormal calcium deposits. Other diagnostic tests include ultrasounds and CT scans, as well as arteriography, and selective venous sampling of the parathyroid blood for PTH levels.
Finally, the treatment of hyperparathyroidism may be grouped into surgical and non-surgical options. The treatment of choice for hyperparathyroidism is parathyroidectomy, which is the surgical removal of one or more of the parathyroid glands.
On the other hand, non-surgical options include diuretic medications like furosemide, which increases the excretion of calcium from the kidneys, along with intravenous hydration by giving large volumes of saline solution. This causes the levels of serum calcium to drop. Now, severe cases of hyperparathyroidism can be treated with the calcimimetic medication cinacalcet, which binds to calcium receptors in the parathyroid glands, increasing their sensitivity to the available calcium in the blood, and ultimately decreasing PTH secretion.