Hyperpituitarism: Nursing
Notes
| HYPERPITUITARISM | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
With hyperpituitarism, hyper- means high, and pituritism refers to the pituitary gland, which is a small, pea-sized gland at the base of the brain that’s made of an anterior lobe, an intermediate lobe and a posterior lobe. So hyperpituitarism describes an excessive secretion or production of one or more of the pituitary hormones, typically those produced by the anterior pituitary.
The anterior lobe, also called the adenohypophysis, contains endocrine cells that produce tropic hormones, which in turn control the secretion of hormones from other endocrine glands or influence a response in target tissues. These include thyroid stimulating hormone, or TSH; adrenocorticotropic hormone, or ACTH; growth hormone, or GH; the gonadotropins, namely follicle stimulating hormone, or FSH, and luteinizing hormone, or LH; prolactin.
So, TSH stimulates thyroid hormone production, which, in turn, increases the basal metabolic rate in all cells. Next, ACTH stimulates adrenal cortisol production, which, in turn, has plenty of effects around the body, such as regulating glucose metabolism, blood pressure, electrolyte balance, and immunity.
Then there’s GH, which stimulates the growth and development of various body tissues, and it also causes release of insulin like growth factor 1, or IGF1, from the liver and skeletal muscles, which mediates the effects of GH on target tissues. Finally, prolactin stimulates lactation during breastfeeding; while FSH and LH influence the function of gonads. All of these hormones are regulated via negative feedback. This means that when a gland, say, the thyroid, secretes more thyroid hormones, this will inhibit TSH levels, in order to maintain the thyroid hormone levels within a normal range.
The posterior lobe, on the other hand, contains hormone-secreting nerve endings extending down from the hypothalamus. The posterior lobe secretes antidiuretic hormone, also called vasopressin or simply ADH, which regulates fluid volume in the body by promoting the reabsorption of water from the urine, making it more concentrated, and it also works as a potent vasoconstrictor. Next is oxytocin, which stimulates uterine contractions during childbirth and causes the breast to push down milk during breastfeeding. Finally, the intermediate lobe, which is the smallest lobe, produces a single hormone called melanocyte stimulating hormone, or MSH for short, which stimulates the production of melanin pigment in skin cells.
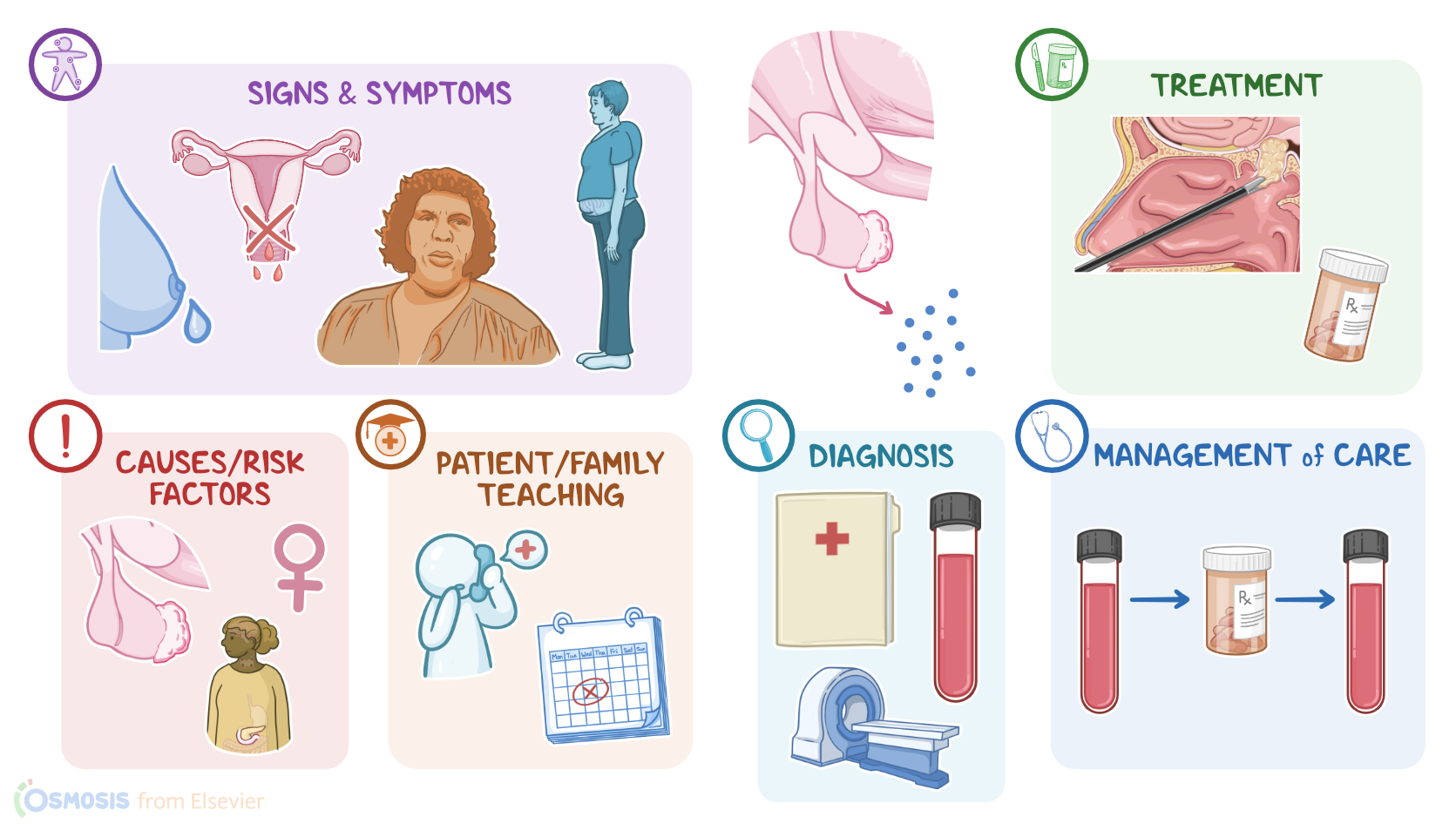
Alright, now the most common cause of hyperpituitarism are benign hormone-secreting pituitary tumors. Other causes of hyperpituitarism include non-pituitary tumors that secrete hormones, and multiple endocrine neoplasia type 1, or MEN1 for short, which is a hereditary condition associated with multiple tumors of the endocrine glands. When it comes to risk factors for hyperpituitarism, these include being assigned female at birth, as well as a family history of hyperpituitarism or MEN1 syndrome.
Regardless of cause, hyperpituitarism leads to excess target-gland secretion of hormones and an increased secretion of target gland hormones and an exacerbation of their effects in the body. So excess TSH causes excess thyroid hormones to be floating around in the body, which sends the basal metabolic rate of all cells into overdrive. We’re talking faster heart beats, faster digestion, and peristalsis, excessive heat generation from intracellular processes, faster transmission of nerve impulses throughout the body, the whole package! With excess GH, there’s increased stimulation for tissue growth and development, which increases skeletal thickness and promotes the growth of extremities; and also increases growth of internal organs and the sweat glands. Finally, with increased prolactin, breast milk production is stimulated even in the absence of pregnancy or breastfeeding. Excess prolactin also interferes with the normal functioning of the gonads.
Clients with hyperpituitarism typically present with signs and symptoms of excess hormone secretion. As a reminder, the three most common clinical scenarios are a result of excess prolactin, GH or ACTH secretion. Excess prolactin can cause galactorrhea, which is a milky discharge from the breasts in absence of pregnancy and breastfeeding; as well as amenorrhea, or absent menstruation, in individuals assigned female at birth; and loss of secondary sexual characteristics, like pubic and axillary hair.
Excess GH, on the other hand, causes signs and symptoms of acromegaly, such as coarse facial details, bigger ears and nose, lower jaw protrusion, enlarged hands and feet, and joint pain. Other features of acromegaly include thickening of the lips, a barrel-shaped chest, and increased sweating.