Hyperthyroidism: Nursing process (ADPIE)
Hyperthyroidism: Nursing process (ADPIE)
Watch later
Watch later
Notes
| HYPERTHYROIDISM | ||
| KEY POINTS | NOTES | |
| PATIENT REPORT |
| |
| PATHOPHYSIOLOGY |
| |
| DIAGNOSIS AND TREATMENT |
| |
| ASSESSMENT |
| |
| NURSING DIAGNOSES |
| |
| PLANNING |
| |
| IMPLEMENTATION |
| |
| EVALUATION |
| |
Transcript
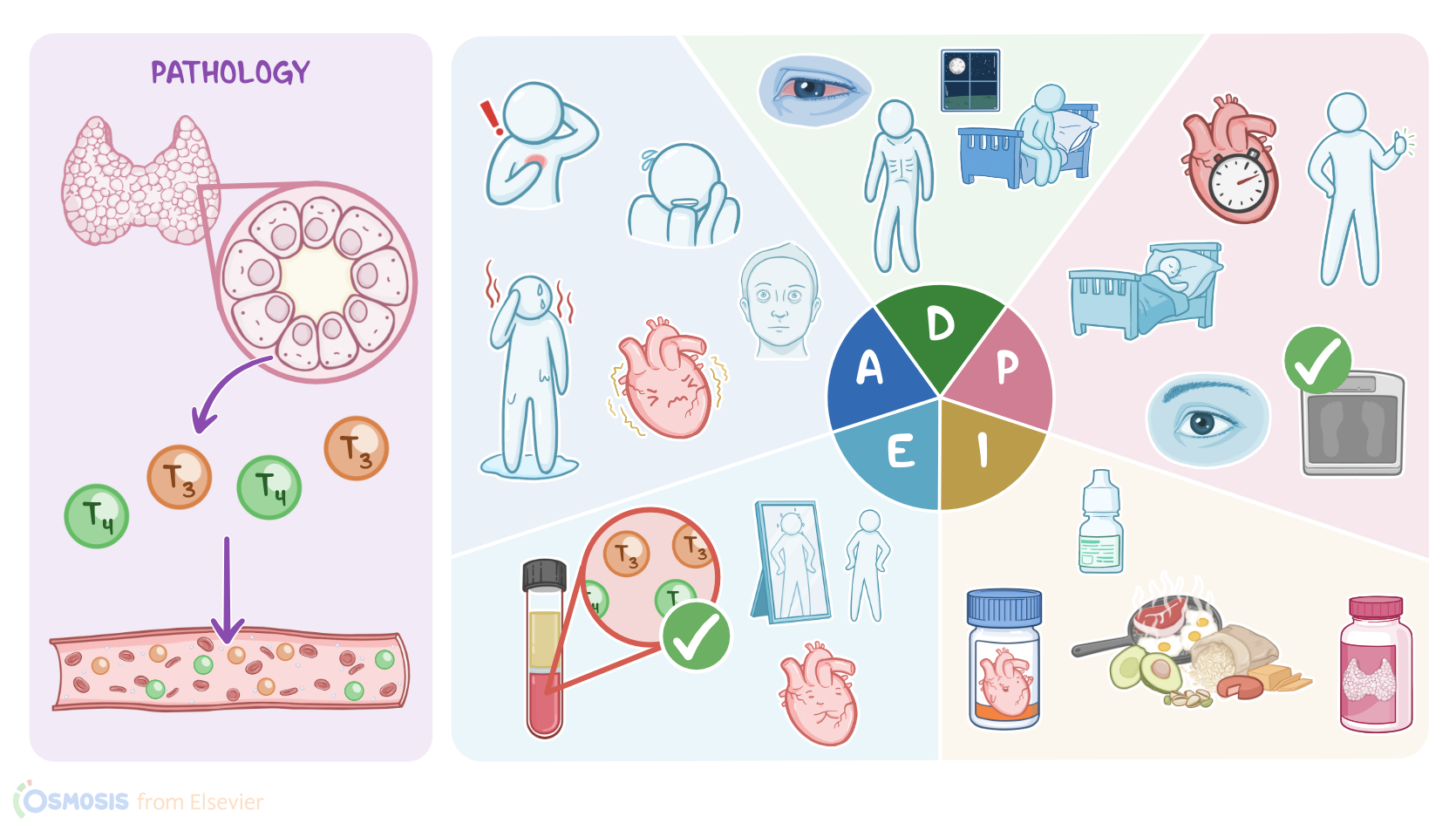
Suzanne Benoit is a 45-year-old female client who presents to her primary care clinic with a report of insomnia, anxiety, and unintentional weight loss. She states she hasn’t felt like herself for the past few weeks, and reports occasional episodes of heart palpitations and hand tremors that she initially thought might be manifestations of panic attacks. After an examination by her physician and a review of laboratory results, Suzanne is diagnosed with primary hyperthyroidism.
Hyperthyroidism is a condition in which the thyroid gland produces and releases excess thyroid hormones. Now, hormonal production is normally regulated by the hypothalamus, which is located at the base of the brain. When the hypothalamus detects low blood levels of thyroid hormones, it releases thyrotropin-releasing hormone, or TRH for short. TRH then stimulates the anterior pituitary gland to release thyroid-stimulating hormone, or TSH, which in turn stimulates hormone production by the thyroid gland, a butterfly-shaped gland located in the neck. The thyroid gland is made up of thousands of thyroid follicles, which release two iodine-containing thyroid hormones, triiodothyronine or T3, and thyroxine or T4, into the bloodstream. These hormones then get picked up by nearly every cell in the body. Once inside the cell, T4 is mostly converted into T3, which is the active form, and it can exert its effect. T3 speeds up the cell’s basal metabolic rate by stimulating protein synthesis, and burning up more energy in the form of sugars and fats. Other effects of thyroid hormones include increasing the cardiac output, stimulating bone resorption, as well as heat production and activating the sympathetic nervous system, which is responsible for our ‘fight-or-flight’ response.
Now, hyperthyroidism occurs when there’s too much thyroid hormone, leading to a hypermetabolic state, in which cellular reactions are happening faster than normal. Hyperthyroidism is usually either primary or secondary. In primary hyperthyroidism, the problem is an overactive thyroid gland. Okay, the most common primary cause is Graves disease, an autoimmune disorder where autoantibodies bind to and activate TSH receptors, which ultimately stimulates the thyroid gland to produce excess thyroid hormones. Another primary cause is toxic nodular goiter, where one or more follicles autonomously start generating lots of thyroid hormone. Next is a hyperfunctioning thyroid adenoma, where the follicular cells start growing uncontrollably, forming a benign tumor that produces excess thyroid hormones. In addition, anytime the thyroid gets damaged or inflamed, like in thyroiditis, there can be a large release of thyroid hormones. On the other hand, in secondary hyperthyroidism, the underlying problem is in the anterior pituitary gland that’s releasing too much TSH. One cause of secondary hyperthyroidism is a TSH-secreting tumor in the anterior pituitary gland, which stimulates a healthy thyroid to produce too much thyroid hormone. Finally, there’s exogenous hyperthyroidism, which is caused by the excessive intake of exogenous thyroid hormones, like the medication levothyroxine.
Now, there are some factors that can put the client at risk of hyperthyroidism. For Graves disease, risk factors include female sex, having a family history of Graves disease, and having another autoimmune disorder like Type 1 diabetes mellitus or primary adrenal insufficiency. For thyroiditis, risk factors include viral upper respiratory tract infection, and pregnancy, which increases the risk for postpartum thyroiditis. Other risk factors for thyroiditis include certain medications like amiodarone or lithium , as well as radiation therapy for cancers in the neck region.
Now, one of the most frequent symptoms of hyperthyroidism is weight loss, despite an increase in appetite, because of the higher basal metabolic rate, as well as diarrhea due to increased gastrointestinal motility. In addition, clients may experience heat intolerance because the body is producing more heat, as well as sweating, hyperactivity, rapid heart rate and palpitations, anxiety, and insomnia because of the effect of thyroid hormones on the sympathetic nervous system. Some clients with hyperthyroidism may present with a neck mass due to an enlarged thyroid, known as goiter. Upon auscultation, a bruit might be heard over a goiter because of the increased blood flow. In females, hyperthyroidism can cause menstrual cycle irregularities, while in males, it can cause erectile dysfunction and gynecomastia, or breast enlargement. Now, there are also unique symptoms to Graves disease, such as Graves’ ophthalmopathy, which occurs due to build-up of glycosaminoglycans, which are carbohydrates that attract water, leading to local swelling around the eyes. This can manifest as exophthalmos, which is anterior bulging of the eyes, as well as chemosis, which is swelling and redness of the conjunctiva. Graves disease can also cause pretibial myxedema, where the skin of the shin becomes swollen, red, and hard.
If not treated, hyperthyroidism can put clients at risk of cardiac complications like heart failure or arrhythmias. Another potential complication is osteoporosis, in which excessive bone resorption results in decreased bone density and increased risk of fractures. In addition, a significant goiter can compress the trachea, causing difficulty breathing. Clients with Graves ophthalmopathy may present with visual impairment, such as double vision, or even vision loss. In addition, exophthalmos can dry out the eyes and increase the risk of corneal ulcers. Finally, untreated hyperthyroidism can lead to thyroid storm, also called acute thyrotoxicosis or thyrotoxic crisis. This is a medical emergency where the body goes into a state of severe hypermetabolism, which can be life threatening. This usually occurs during periods of acute stress such as infections, trauma and surgery, and presents with more severe symptoms of hyperthyroidism, as well as fever, arrhythmia, seizures, impaired consciousness, and possibly coma.
Diagnosis of hyperthyroidism can be done based on history and clinical findings. Next, the diagnosis can be confirmed by measuring blood levels of TSH, T3, and T4. In primary hyperthyroidism, T3 and T4 will be high, while TSH will be low due to the negative feedback inhibition exerted by the increased thyroid hormones on the anterior pituitary gland. On the other hand, secondary hyperthyroidism that’s caused by an anterior pituitary gland tumor, will result in high or normal TSH, and high T3 and T4. Other tests include a radioactive iodine uptake test and a thyroid scan, which help determine the specific cause of the hyperthyroidism. For example, in Graves disease, the scan will show a diffuse and generalized uptake of radioactive iodine across the thyroid gland; whereas toxic nodular goiter and adenoma would present with a localized uptake; and thyroiditis, would result in decreased thyroid uptake of radioactive iodine as the gland’s follicles are actually destroyed. Finally, an electrocardiograph, or ECG, can be done to assess for cardiac complications.
Treatment varies based on the exact cause of hyperthyroidism, but generally involves medications like beta-blockers, such as propranulol propranolol, which rapidly decreases the symptoms. In addition, clients may also get corticosteeroids corticosteroids like prednisolone to inhibit conversion of T4 to T3, as well as antithyroid medications, like propylthiouracil and methimazole, which decrease thyroid hormone synthesis. Thyroid hormone synthesis can also be decreased with potassium iodide, also called Lugol solution. However, this is rarely used. In some cases, radioactive iodine ablation can be performed to partially or completely destroy thyroid function, followed by replacement hormone therapy. Finally, in clients with severe symptoms or a significant goiter, surgery can be done to remove the thyroid gland partially or completely via thyroidectomy.