Impetigo: Nursing
Notes
| IMPETIGO | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
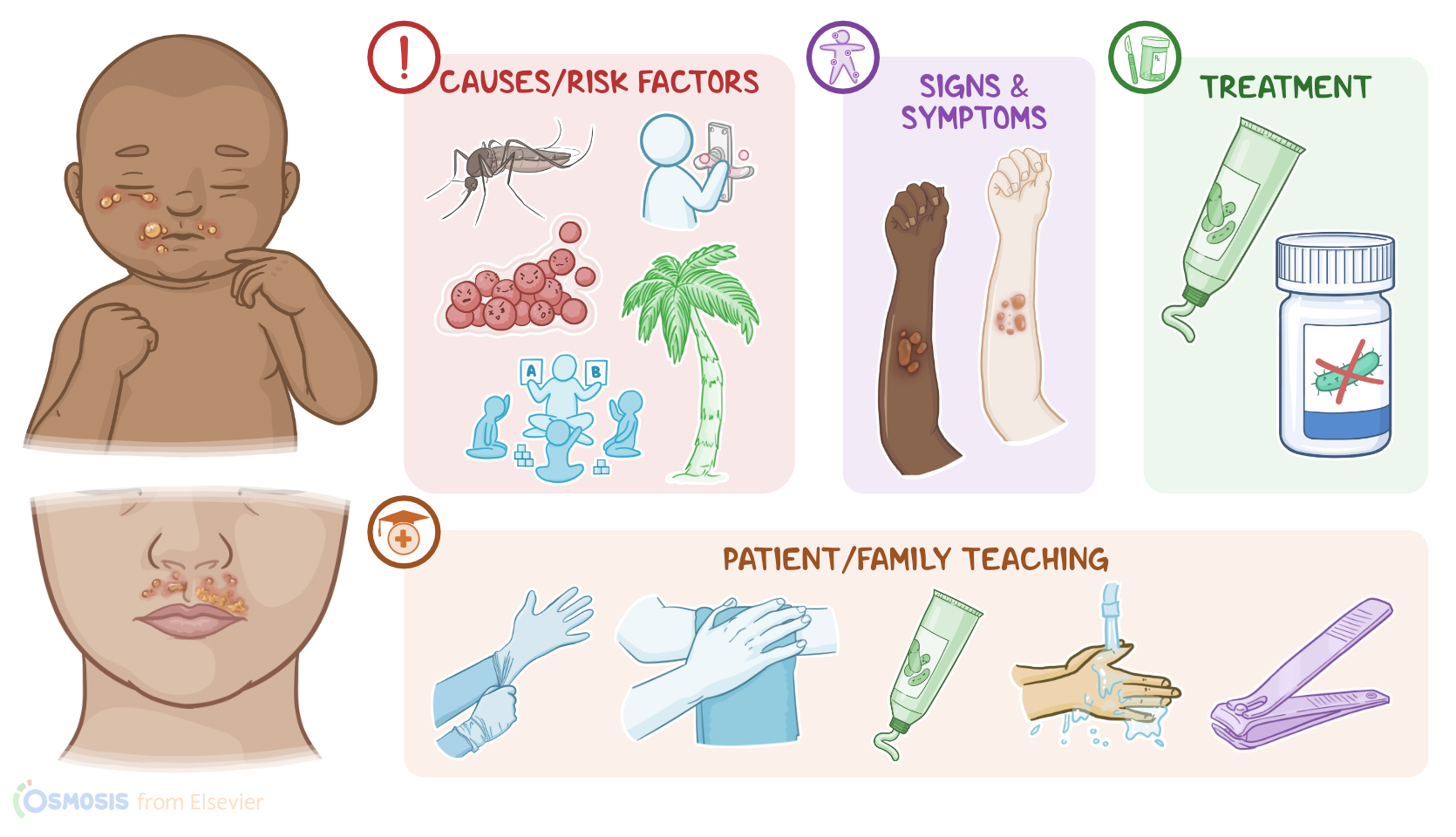
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Impetigo is a superficial and highly contagious bacterial skin infection, most often affecting young children between the ages of 2 and 5 years, and is more common during warm, humid months of the year.
Alright, let’s go over some physiology. Normally, the skin surface is colonized by a huge number of microorganisms that make up the normal skin flora. This flora consists mostly of bacteria, such as Staphylococcus epidermidis, as well as certain fungi, such as Candida albicans. The normal skin flora is typically non-pathogenic, meaning that these microorganisms don’t cause any disease. In fact, they are often beneficial, since they serve as a physical and competitive barrier that helps prevent pathogenic microorganisms from invading and infecting the skin.
Now, impetigo is a bacterial skin infection that’s typically caused by Gram positive pathogenic bacteria like Staphylococcus aureus or Streptococcus pyogenes. In addition, there’s an increasing number of impetigo cases caused by antibiotic-resistant strains, such as methicillin-resistant Staphylococcus aureus or MRSA for short, as well as gentamicin-resistant Staphylococcus aureus.
Typically, the infection is transmitted from person to person through direct contact with skin lesions. Less frequently, the infection can be transmitted indirectly when a client touches a contaminated surface, such as clothing or bed linens. Common places where impetigo spreads include daycare centers, nursing homes, or schools.
Now, risk factors that can disrupt the normal skin flora include living in a warm, humid climate, as well as having poor hygiene, and underlying conditions like diabetes or a weakened immune system. Additional risk factors that can allow these bacteria to invade the skin include having previous damage due to insect bites, minor trauma, abrasions, or skin conditions like eczema or psoriasis.
Now, the infection can be classified as primary impetigo when it occurs on intact skin, or secondary impetigo when it occurs in previously damaged skin, like with insect bites, abrasions, or in infected chickenpox lesions. Regardless of the type, pathogenic bacteria invade the skin and cause an infection. In addition, some of these bacteria can produce exfoliative toxins that further damage the skin, or a secondary infection can occur, potentially causing complications such as cellulitis, or rarely, acute glomerulonephritis.
Now, depending on its clinical manifestations, impetigo can be classified as non-bullous or bullous. The most common type is non-bullous impetigo, which usually occurs on areas of compromised skin integrity, most often involving the skin around the nose and mouth, as well as the neck and extremities. These lesions appear as vesicles or pustules, which then rupture in 1 to 2 days and form characteristic honey-colored, or golden, crusts around an erythematous, moist base. Clients may also experience itching or a burning sensation, and may present with regional lymphadenopathy.
On the other hand, bullous impetigo usually appears on intact skin, most often involving the trunk, as well as moist intertriginous areas where two skin surfaces rub together, such as the axillae and groin folds. These lesions appear as bullae filled with clear yellow fluid that develops into an opaque, dark yellow or purulent fluid. Now, these bullae can rupture easily, leaving a thin brown crust behind. Less commonly, clients may also present with systemic symptoms like fever, chills, and malaise.
Impetigo is typically diagnosed based on the client’s history and physical assessment. Laboratory tests are not routinely performed, but in unclear cases, a Gram stain or culture of a lesion swab can confirm the diagnosis.