Irritable bowel syndrome (IBS): Nursing
Notes
| IRRITABLE BOWEL SYNDROME | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Irritable bowel syndrome, or IBS for short, is a condition characterized by irregular intestinal motility. Based on the associated symptoms it can fall into three groups: IBS - C, which is associated with constipation; IBS - D, which is associated with diarrhea; IBS - M, which is mixed, meaning that it is associated with alternating bouts of constipation and diarrhea; and IBS unclassified, meaning the IBS can’t be classified into one of the other subtypes.
All right, now, let’s zoom into the wall of the intestine, which is made up of four layers. The outermost layer is called serosa or adventitia and is a connective tissue that binds the intestine to the surrounding structures. Next is the muscular layer, which houses three smooth muscle layers. These muscles contract and relax in a rhythmic way to produce wave-like movements of the intestines, called peristalsis, which propel the food down the gastrointestinal tract. The contractions of these muscles are controlled by a mini nervous system that lies within the walls of the intestines. Typically, this system works on its own, but it is also affected by the sympathetic and parasympathetic nervous systems.
After that is the submucosa, which consists of a dense layer of tissue that contains blood vessels, lymphatics, and nerves. And finally, there’s the innermost layer, called the mucosa, which consists of simple columnar epithelium spanned by goblet cells. This mucosa forms invaginations called colonic crypts or glands.
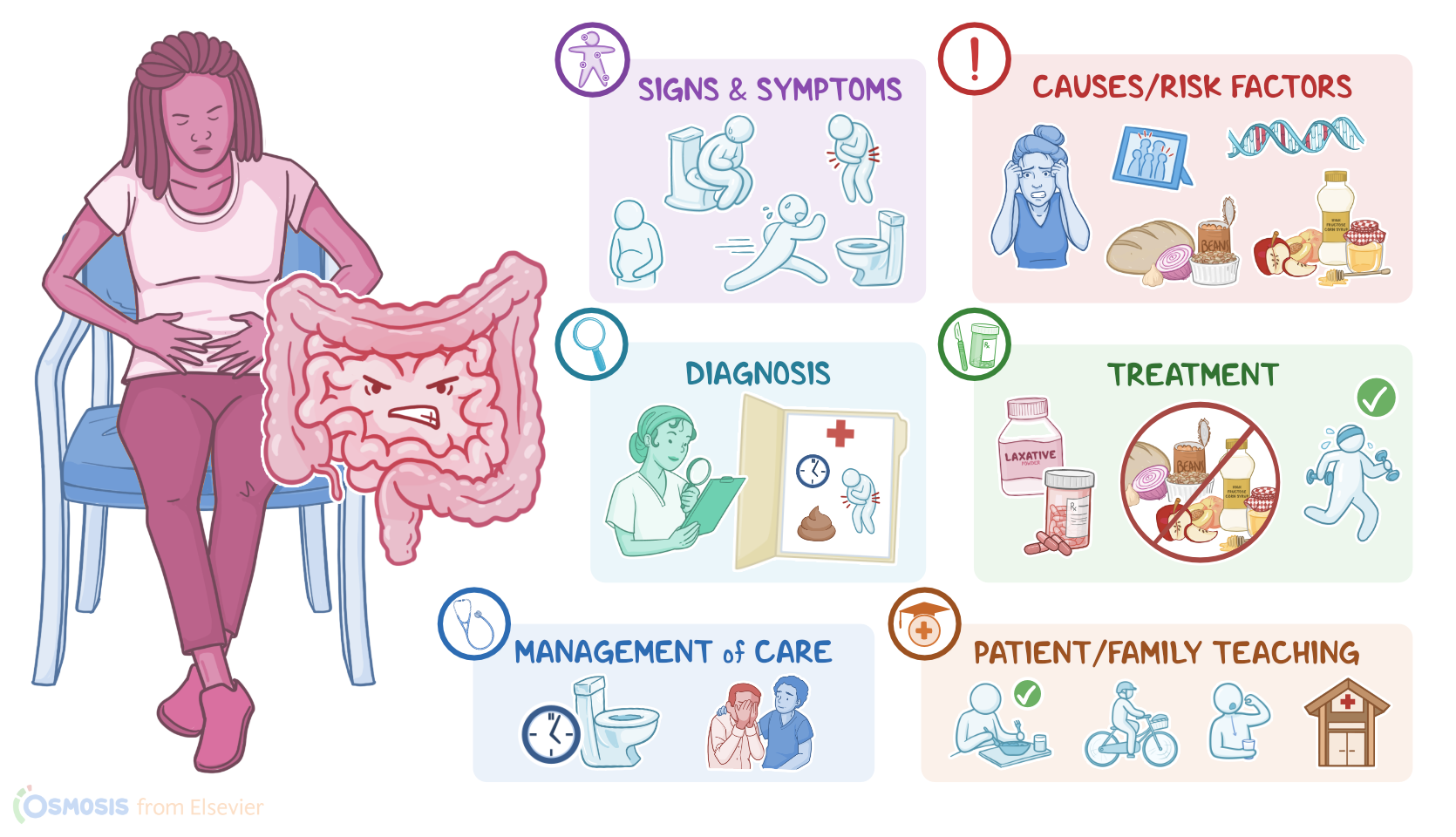
Now, there isn’t a single cause of irritable bowel syndrome, but rather it’s a multifactorial disease, meaning that there’s a combination of risk factors and dietary triggers. These include genetic predisposition and family history, as well as an age below 50, or being assigned female at birth. Additional risk factors include gastrointestinal conditions, such as previous gastrointestinal infections, alterations in the fecal microflora, hypersensitivity of visceral receptors in the wall of the gut; as well as psychological conditions, such as stress, anxiety, post-traumatic stress disorder or PTSD, and depression.
On the other hand, the main dietary triggers include carbohydrates like fermentable oligosaccharides, disaccharides, monosaccharides, and polyols, also known as FODMAPs, which are poorly absorbed in the small intestine and tend to ferment in the colon. FODMAPs can be found in foods such as dairy products, certain fruits like apples, avocados or cherries; garlic and onions; beans and legumes; wheat; and sweeteners like honey, high fructose corn syrup, and sugar alcohols.
All right, now, regardless of what triggers the disease, there is an alteration in the gastrointestinal motility, causing the food to pass quickly through the intestines, leading to diarrhea. In other cases, these impulses may also decrease intestinal motility, causing constipation.
Typically, clients with irritable bowel syndrome present with changes in bowel habits, including constipation, diarrhea, or both. They may also experience recurrent abdominal pain which often improves with bowel movement, as well as bloating, and mucous in the stool. In addition, non-gastrointestinal symptoms are often present, including headache, sleep issues, and fatigue.
The diagnosis of irritable bowel syndrome is mainly based on the client’s history and physical assessment. Specifically, there’s a set of criteria, known as Rome IV criteria,which looks at timing and frequency of symptoms, presence of abdominal pain, as well as a change in stool frequency and change in stool shape. Additional diagnostic tests such as colonoscopy can be also used to rule out other disorders, like colorectal cancer; as well as abdominal X-rays to check for stool accumulation.
Now, the treatment of IBS focuses on relieving the symptoms associated with each type of IBS. For example, constipation in IBS - C can be treated with fiber supplements, such as bulk-forming agents like psyllium, in addition to laxatives like polyethylene glycol, or gastrointestinal agents like lubiprostone, or linaclotide. On the other hand, diarrhea in IBS - D can be treated with antidiarrheal medications like loperamide. Also, medications that reduce motility, like eluxadoline, and antispasmodic medications, like hyoscyamine, are often used. In mixed types of IBS, clients may take laxatives or antidiarrheals as needed. Finally, there are certain medications that are often used to support clients with any type of IBS, including rifaximin for bloating, eluxadoline for abdominal pain, and tricyclic antidepressants for associated mood symptoms.