Persistent pulmonary hypertension of the newborn (PPHN): Nursing
Notes
| PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN (PPHN) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
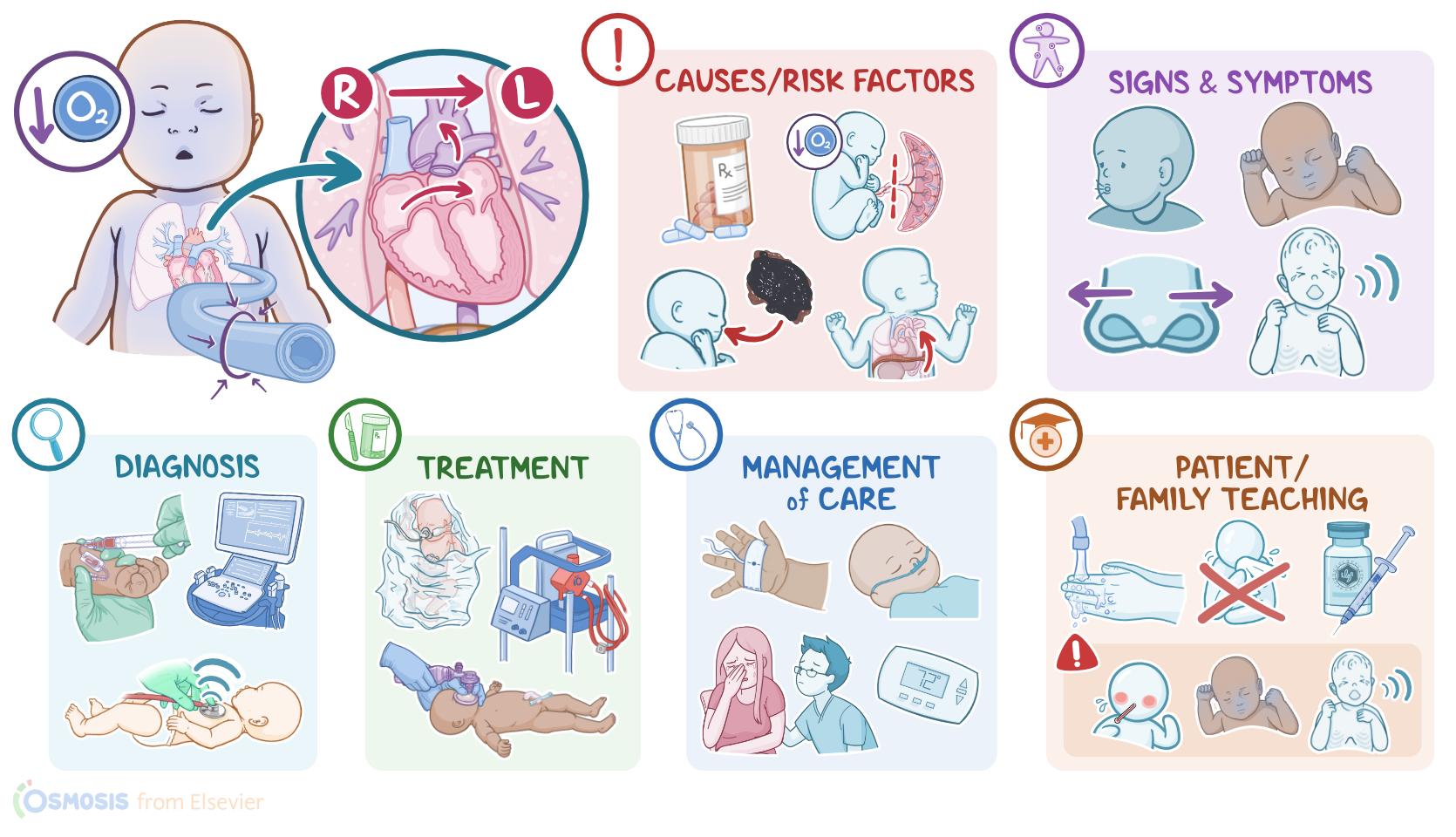
Persistent pulmonary hypertension of the newborn, or PPHN for short, is a condition in which the pulmonary arteries remain constricted after birth, resulting in increased pulmonary vascular resistance and right-to-left shunting of blood, ultimately leading to hypoxemia and acidosis.
Alright, let’s quickly recap the physiology of pulmonary blood vessels. During intrauterine life, the fetal lungs are filled with fluid and the arteries are tightly constricted, so the pressure in the fetal lungs is high, and in the fetal heart, the pressure on the right side is higher than on the left side of the heart. This pressure difference between the right and left side of the heart allows the majority of the oxygenated blood coming from the placenta to the right atrium to bypass the lungs and pass directly through the foramen ovale, which is an opening between the two atria, into the left atrium. At the same time, the right ventricle pumps blood into the pulmonary trunk. Again, since the lungs are collapsed, most blood flows through the ductus arteriosus into the descending aorta and eventually to the umbilical arteries that lead to the placenta.
Now, after birth, when the baby takes its first breath, their lungs expand and pulmonary blood flow increases. This makes pulmonary vessels expand, and decreases pulmonary blood pressure. In turn, this decreases the pressure in the right side of the heart, which causes the foramen ovale to close. As the baby continues to breathe, arterial oxygen levels increase, causing the ductus arteriosus to constrict. The process of closing these shunts is gradual and may take up to 48 hours to fully close. Deoxygenated blood can then flow into the lungs to get oxygenated, and the newborn circulation is established.
Now, the exact cause of PPHN is unknown, but it's believed to be associated with risk factors that can interfere with the development of the lungs. These include the maternal use of certain medications, such as nonsteroidal antiinflammatory medications, or NSAIDs, and selective serotonin reuptake inhibitors, or SSRIs for short. Another risk factor is hypoxemia, or low oxygen levels in the blood, before, during, or after birth. This can be a result of asphyxia, where oxygen supply to the fetus or newborn is cut off; meconium aspiration syndrome, where the meconium or first stool of the newborn, enters the respiratory tract causing obstruction and distress; as well as congenital diaphragmatic hernia, in which an opening in the diaphragm allows the abdominal organs to herniate into the thorax pushing against the lungs.
Hypoxemia can also be the result of hypothermia and sepsis, as well as polycythemia, in which the increased number of red blood cells causes a sluggish blood flow leading to tissue hypoxia and ischemia. Finally, congenital heart disease, like pulmonary atresia or tricuspid atresia may lead to decreased blood flow and underdevelopment of pulmonary vessels.
Okay, now the pathology of PPHN typically starts with hypoxemia, which causes the pulmonary artery and its branches to stay constricted even after birth. This means that the blood pressure in the pulmonary circulation, and the right side of the heart do not decrease as they should after birth and remain increased compared to the left side of the heart, creating a right-to-left shunt through the fetal shunts. So, deoxygenated blood coming from the various tissues around the body into the right atrium bypasses the lungs and goes straight through the foramen ovale and ductus arteriosus to the left side of the circulation. From there, deoxygenated blood returns back to the tissues. This being said, tissues around the body cannot get enough oxygen, so they have to rely on anaerobic metabolism which produces lactic acid, resulting in metabolic acidosis. Acidosis also accentuates pulmonary vasoconstriction, further increasing pulmonary blood pressure and right-to-left shunting, and creating a vicious cycle of hypoxemia.
Ultimately, persistent hypoxemia may lead to complications like organ damage and sensorineural hearing loss, in addition to neurodevelopmental and cognitive delay.
Newborns with PPHN typically present with signs of respiratory distress, including nasal flaring, tachypnea, and intercostal or substernal retractions during inspiration, along with grunting during expiration. The infant will often appear cyanotic, due to the deoxygenated blood in the systemic circulation.
The diagnosis of PPHN starts with a history and physical assessment, followed by arterial blood gas, or ABG analysis, which shows hypoxemia and metabolic acidosis. A low PaO2 persisting despite administration of a high oxygen concentration is also often found in PPHN, as well as a higher preductal oxygen saturation than a postductal oxygen saturation. Upon auscultation, a systolic murmur might be heard, usually from a patent ductus arteriosus.To confirm the diagnosis, an echocardiography is typically performed, which shows elevated pressures in the pulmonary arteries and right-to-left shunting of blood through the foramen ovale and ductus arteriosus.
The treatment of PPHN starts with addressing the underlying cause of hypoxemia, along with supportive measures, including the administration of warm, humidified oxygen; continuous positive airway pressure or CPAP, using face masks or nasal prongs; as well as inhaled nitric oxide, which help dilate the pulmonary blood vessels, and decrease pulmonary blood pressure. If needed, sedation, and high-frequency ventilation might be also used. Finally, in severe cases, extracorporeal membrane oxygenation, or ECMO, which is a machine that temporarily replaces the function of the heart and lung, might be required.
Okay, let’s look at the nursing care you’ll be providing to an infant with persistent pulmonary hypertension of the newborn. Your priority nursing goals are to optimize oxygenation and provide emotional support.
Begin by administering the prescribed supplemental oxygen and instituting pulse oximetry. Collaborate with respiratory therapy to keep the oxygen saturation within the prescribed parameters by instituting a CPAP, inhaled nitric oxide, or intubation mechanical ventilation, as indicated.