Preeclampsia and eclampsia: Nursing
Preeclampsia and eclampsia: Nursing
Acute Final
Acute Final
Notes
| PREECLAMPSIA AND ECLAMPSIA | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
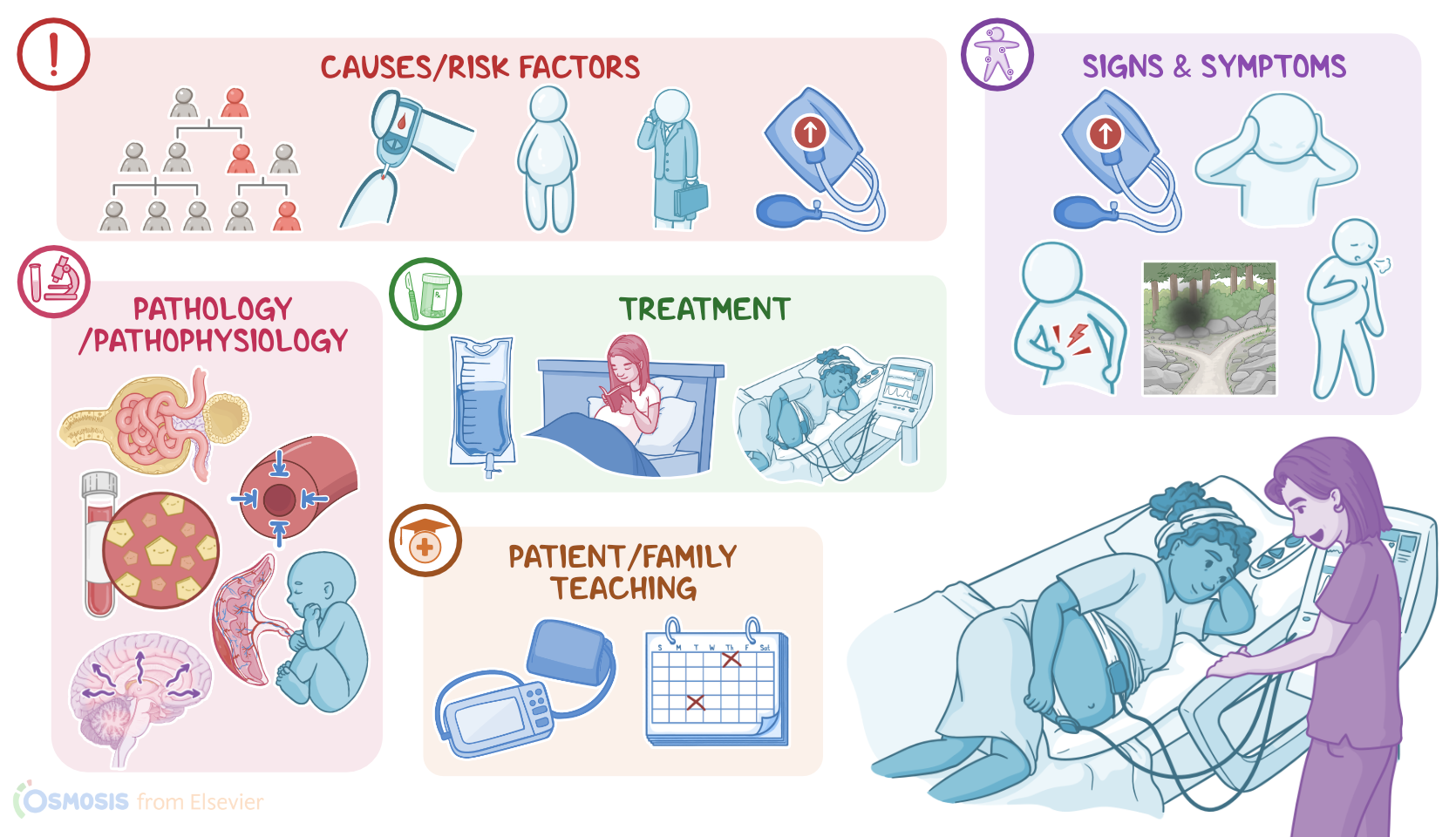
Preeclampsia is a pregnancy-specific condition characterized by new-onset hypertension and proteinuria after 20 weeks of gestation or during the postpartum period in a previously normotensive client; while eclampsia is when a client with preeclampsia develops generalized seizures. These two conditions differ from gestational hypertension, which simply refers to new onset of hypertension during pregnancy, without proteinuria or seizures.
Now, let’s quickly review the physiology of blood pressure regulation during pregnancy. There are three key factors to keep in mind: cardiac output, which is the amount of blood that the heart pumps out to the systemic circulation in a minute; intravascular volume, which is the amount of blood in the client’s circulation; and peripheral vascular resistance, which is the resistance of blood flow in peripheral arteries, and is regulated via vasoconstriction or vasodilation as needed. Remember that in pregnant clients, the cardiac output and intravascular volume increase, but the peripheral vascular resistance decreases.
That’s because during pregnancy, there’s a relative decrease in the response to vasoconstrictor molecules, like angiotensin II, and there are also higher levels of vasodilator molecules, like prostacyclin PGI2. As a result, blood vessels dilate more to accommodate the increased blood volume, and this keeps blood pressure in the normal range, below 120 over 80 mmHg.
This increased blood volume can come in pretty handy, especially since the placenta needs a lot of blood. Remember that the placenta is a temporary organ that develops in the uterus during pregnancy, and connects the pregnant client with the fetus. The way this works is that a type of endometrial arteries called the spiral arteries dilate during pregnancy, and open into the placenta to form little pools of blood. On the fetal end, the umbilical vein connects to the placenta and also opens into those pools. This way the umbilical vein can get nutrient and oxygen-rich blood for the fetus without it being in direct contact with the spiral arteries. In the same vein, pun intended, deoxygenated blood and waste products from the fetus are carried to the placenta by the umbilical arteries, and from there, they are picked up by the pregnant client’s veins to be eliminated.
That being said, while the exact cause of preeclampsia and eclampsia is unknown, some risk factors for developing these conditions have been identified. These include family history of preeclampsia, first pregnancy or being over 35 years of age, as well as obesity, chronic hypertension or diabetes before pregnancy, and Black race.
Now, the pathology of preeclampsia and eclampsia is thought to develop in clients that are particularly sensitive to vasoconstrictor molecules like angiotensin II, and they also seem to have lower levels of vasodilating molecules like prostacyclin PGI2. As a result, these clients have increased peripheral vascular resistance and low blood flow to target organs, like the placenta, as well as the kidneys, liver, and brain.
On the placenta end, decreased perfusion can cause the release of proinflammatory cytokines and, as a consequence, systemic inflammation. Another element that can play a role in decreased placental perfusion can be the aberrant development of spiral arteries, which also plays a role in systemic inflammation. Either way, low blood flow to the placenta means low blood flow to the developing fetus, which can cause intrauterine growth restriction, low birth weight, preterm birth or even fetal death. Additionally, with preeclampsia, there’s also an increased risk of placental abruption, meaning the placenta prematurely detaches from the uterine wall.
On the kidney end, low blood flow can damage the tiny glomeruli that normally work to keep blood proteins from making their way into the urine; so this results in proteinuria. As a consequence, less proteins in the blood can cause generalized or localized edema, like pulmonary edema. Additionally, over time, low renal blood flow can also lead to renal insufficiency.
On the liver end, decreased blood flow can cause liver damage and dysfunction. And because the liver is in charge of conjugating bilirubin to produce bile, some clients may develop hyperbilirubinemia. In addition, the liver is full of enzymes for various metabolic processes, the damaged liver may release these enzymes into the blood.
And let’s not forget about the brain! Now, the exact mechanism of brain damage during preeclampsia is not understood, but it appears to be twofold. On the one hand, the vasoconstriction of cerebral blood vessels means they can’t withstand the increased blood pressure, so the tiniest of cerebral blood vessels are at risk of rupturing and causing cerebral hemorrhage and stroke. On the other hand, inflammation and high blood pressure can alter the normal physiology of cerebral circulation, and cause cerebral edema and small areas of cerebral ischemia. This could play a role in the development of seizures and the progression of preeclampsia to eclampsia.
Okay, now, the clinical manifestations of preeclampsia and eclampsia can vary, but they include hypertension, defined as systolic blood pressure over 140 mmHg, diastolic blood pressure over 90 mmHg, or both. Most clients also develop proteinuria, and some might develop dyspnea as a result of pulmonary edema.
Now, features of severe disease are defined as having systolic blood pressure over 160 mmHg, or diastolic blood pressure over 110 mmHg; or signs of end-organ damage, such as decreased urinary output, which can indicate renal damage; jaundice and right upper quadrant or epigastric pain, which can indicate liver damage; and visual disturbances, such as blurry or double vision; scotomata, which means “seeing spots”, as well as headache, confusion, drowsiness, numbness and tingling, or hyperreflexia, which can indicate brain damage. Finally, if preeclampsia progresses to eclampsia, the client can develop seizures, which can occur before, during, or sometimes even after labor.
The diagnosis of preeclampsia and eclampsia starts with the client’s history and physical assessment confirming hypertension; followed by laboratory tests showing proteinuria. In some cases, preeclampsia can be diagnosed in the absence of proteinuria if there is evidence of end-organ damage. Some laboratory cues for end-organ damage can include elevated creatinine blood levels, hyperbilirubinemia, elevated liver enzymes, and thrombocytopenia or low platelets. When elevated liver enzymes and thrombocytopenia occur alongside hemolytic anemia, that could indicate a potentially life-threatening complication in pregnancy called HELLP syndrome, which stands for Hemolysis, Elevated Liver enzymes, and Low Platelets.