Rocky Mountain spotted fever (RMSF): Nursing
Notes
| ROCKY MOUNTAIN SPOTTED FEVER | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
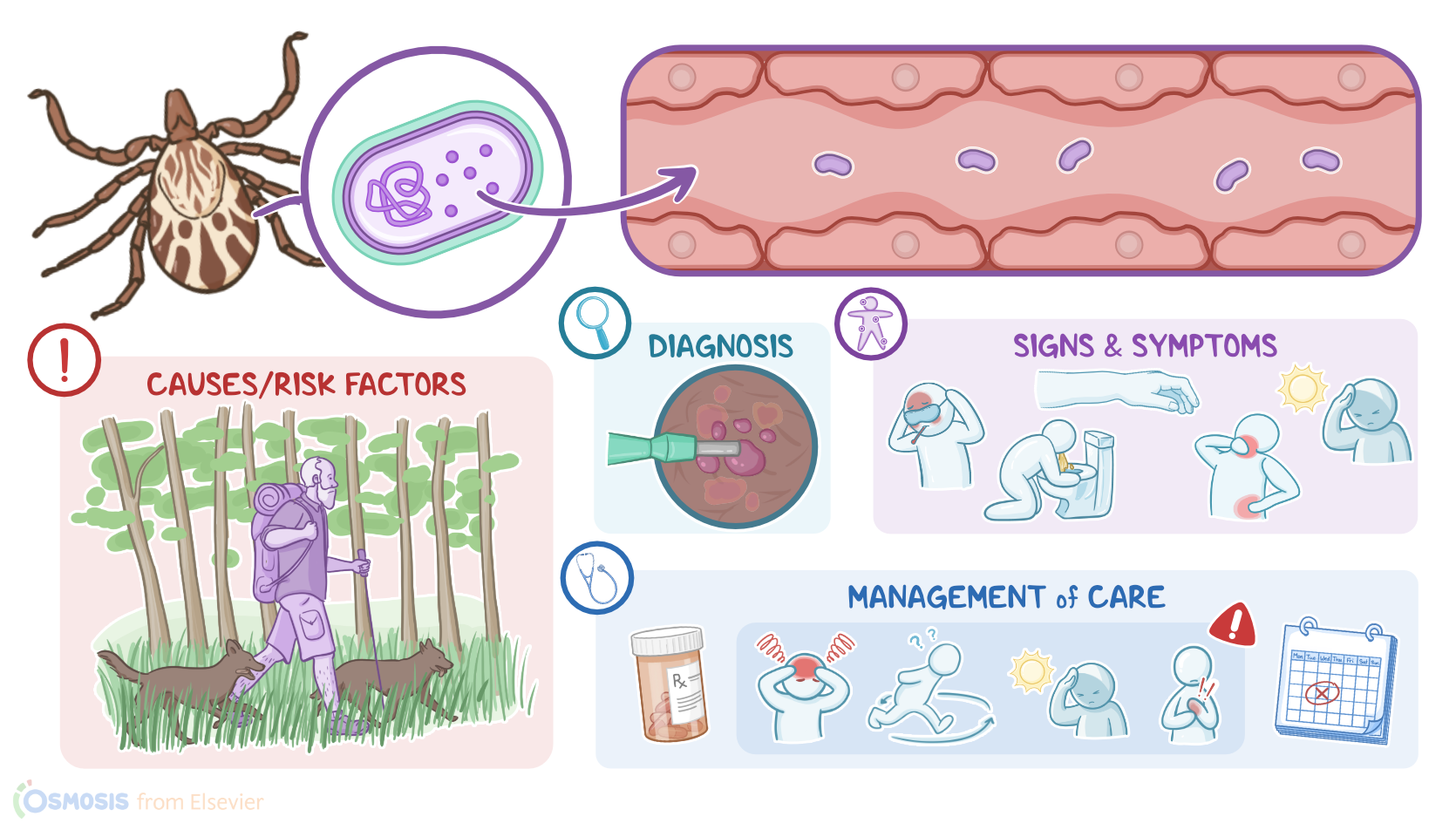
Rocky Mountain spotted fever is a tick-borne, infectious disease caused by the bacteria Rickettsia rickettsii, which are endemic in the Midwestern, Northeastern. and south Atlantic and south-central regions of the United States. The organism primarily attacks the endothelial cells lining the inside of small blood vessels causing small vessel vasculitis, or inflammation of small blood vessels. If not treated promptly, the disease can be fatal.
Alright, first let’s quickly review some physiology. The endothelium consists of a single layer of endothelial cells that line the inside of the entire circulatory system, from the heart to the smallest blood vessels supplying the various organ systems. In addition to being a protective barrier, the endothelium plays a major role in the regulation of the vascular tone by releasing vasoconstrictive and vasodilatory substances, while it is also an important regulator of inflammation.
During an inflammatory response, the endothelial cells contribute to the release of small proteins, called cytokines, and other proinflammatory molecules that help modulate the activity of other immune cells, as well as promote the adhesion of immune cells, called leukocytes, to the endothelium, thereby facilitating their migration to the site of inflammation. Finally, the endothelium also helps to regulate blood flow, platelet aggregation, and blood clotting.
Okay, now Rocky Mountain spotted fever is caused by the obligate intracellular, Gram negative bacterium Rickettsia rickettsii. The infection is transmitted to humans through vectors primarily through the bite of an infected tick, like Dermacentor variabilis, or the American dog tick, which can be found in Eastern and South-central US; Dermacentor andersoni, or the Rocky Mountain wood tick, which can be found west of Mississippi River; and Rhipicephalus sanguineus, or the common brown dog tick, which can be found in Southwestern US.
Now, the infection is more common during the active tick season, which lasts from May to September, but can occur anytime during the year in places where the weather is warm. Since ticks like to live in warm, humid environments, they are usually found in forested areas with wood, bushes, and tall grass. Risk factors for this disease include living in endemic areas or traveling there, especially during spring and summer; living near wooded areas or areas with high grass; and frequent exposure to dogs.
Alright, after entering the body through the bite of an infected tick, Rickettsia rickettsii spreads through the body via the blood and attaches to endothelial cells lining the inside of small blood vessels. Rickettsiae then invade endothelial cells, replicate inside them, and spread from cell to cell causing endothelial cell injury. Now, an important consequence of endothelial cell injury is increased vascular permeability, meaning that the small blood vessels dilate and become more permeable, allowing plasma proteins, such as albumin, and fluid to leak from the vessel lumen into the interstitial tissue. This results in edema, or expansion of the interstitial fluid volume; hypovolemia, that can lead to hypotension, and hypoalbuminemia, or reduced levels of albumin in the blood.
Additionally, endothelial cell injury stimulates an immune response resulting in small vessel vasculitis, which can lead to vascular injury in the organs supplied by these small vessels, including the lungs, heart, brain, skin, and kidneys. Moreover, small vessel vasculitis can result in activation of circulating platelets to generate thrombin, and trigger the coagulation system, leading to thrombi formation and in severe cases, small-vessel occlusion and necrosis.
Unfortunately, if not treated promptly, Rocky Mountain spotted fever can lead to several complications, including disseminated intravascular coagulation, which is a life-threatening condition characterized by both accelerated clotting and uncontrollable bleeding; pulmonary edema; acute renal failure; meningitis; encephalitis; and multi-organ dysfunction, which can ultimately result in death. Other potential complications include hearing and vision loss.
Now, after the initial tick bite, there’s an incubation period of 2 to 14 days. Then, early symptoms start to appear, including nonspecific flu-like symptoms such as fever, headache, malaise, and myalgias. Later on, an erythematous rash appears starting from the wrists and ankles and spreading to the trunk, palms and soles. The rash is maculopapular, meaning that it consists of macules, or small, flat, pink, non-itchy spots, and papules, which are raised areas of skin. The rash is also blanching, meaning that it turns pale if pressure is applied to it.
Eventually, the maculopapular rash may turn into petechial, or hemorrhagic, characterized by small red or purple spots on the skin. In severe cases, some areas of skin may become necrotic, especially in regions supplied by terminal arteries, such as the fingers, toes, nose, ears and genitals.
Other common manifestations of Rocky Mountain spotted fever include ankle and wrist swelling, and gastrointestinal symptoms, including anorexia, nausea, vomiting, and abdominal pain. Individuals may also develop signs and neurological symptoms such as photophobia, confusion, and lethargy. If the infection is left untreated, clients may also experience shock with multi-organ dysfunction.
The diagnosis of Rocky Mountain spotted fever starts with the client’s history, which could include recent activities such as hiking, camping, or hunting in areas with high grass, weeds, and brush; along with physical assessment. Diagnosis can be confirmed with the detection of IgG antibodies based on an indirect immunofluorescence assay, or IFA, test using Rickettsia rickettsii antigen.
Also, since Rickettsiae cannot be cultured in most clinical laboratories, diagnosis can also be confirmed with the detection of Rickettsia rickettsii DNA on a skin biopsy specimen, or a blood sample using polymerase chain reaction, or PCR assay. Alternatively, immunohistochemical staining of the organism on a skin biopsy specimen can be done. A complete blood count typically shows normal white blood cell count and decreased platelets. Lab results can also show hyponatremia and liver dysfunction.