Shock - Anaphylactic: Nursing
Shock - Anaphylactic: Nursing
Medical Surgical
Medical Surgical
Notes
| SHOCK - ANAPHYLACTIC | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
Shock is a life-threatening condition that occurs when body organs don’t receive enough oxygen and nutrients to function properly. Shock can be grouped into four types based on the cause: hypovolemic, cardiogenic, obstructive, and distributive shock, which can be further divided into septic, anaphylactic, and neurogenic shock. Now, to understand anaphylactic shock, let’s quickly review the physiology of blood vessels, which contain smooth muscle in their walls. When the smooth muscle relaxes, it increases the diameter of blood vessels, called vasodilation. On the other hand, when smooth muscle contracts, the diameter of blood vessels decreases, called vasoconstriction.
The contraction and relaxation of smooth muscles are primarily controlled by the sympathetic nervous system, which normally maintains a partial constriction, generating enough force to keep blood moving through the circulatory system. The sympathetic system stimulation can increase or decrease to keep up with the body’s needs. Increased sympathetic stimulation of the blood vessels causes vasoconstriction and increases peripheral vascular resistance. Vasoconstriction, when the total blood volume is constant, raises blood pressure and allows blood to flow faster through the blood vessels. In contrast, vasodilation is typically caused by decreased sympathetic stimulation, in addition to inflammatory cytokines and histamine, which decrease peripheral vascular resistance.
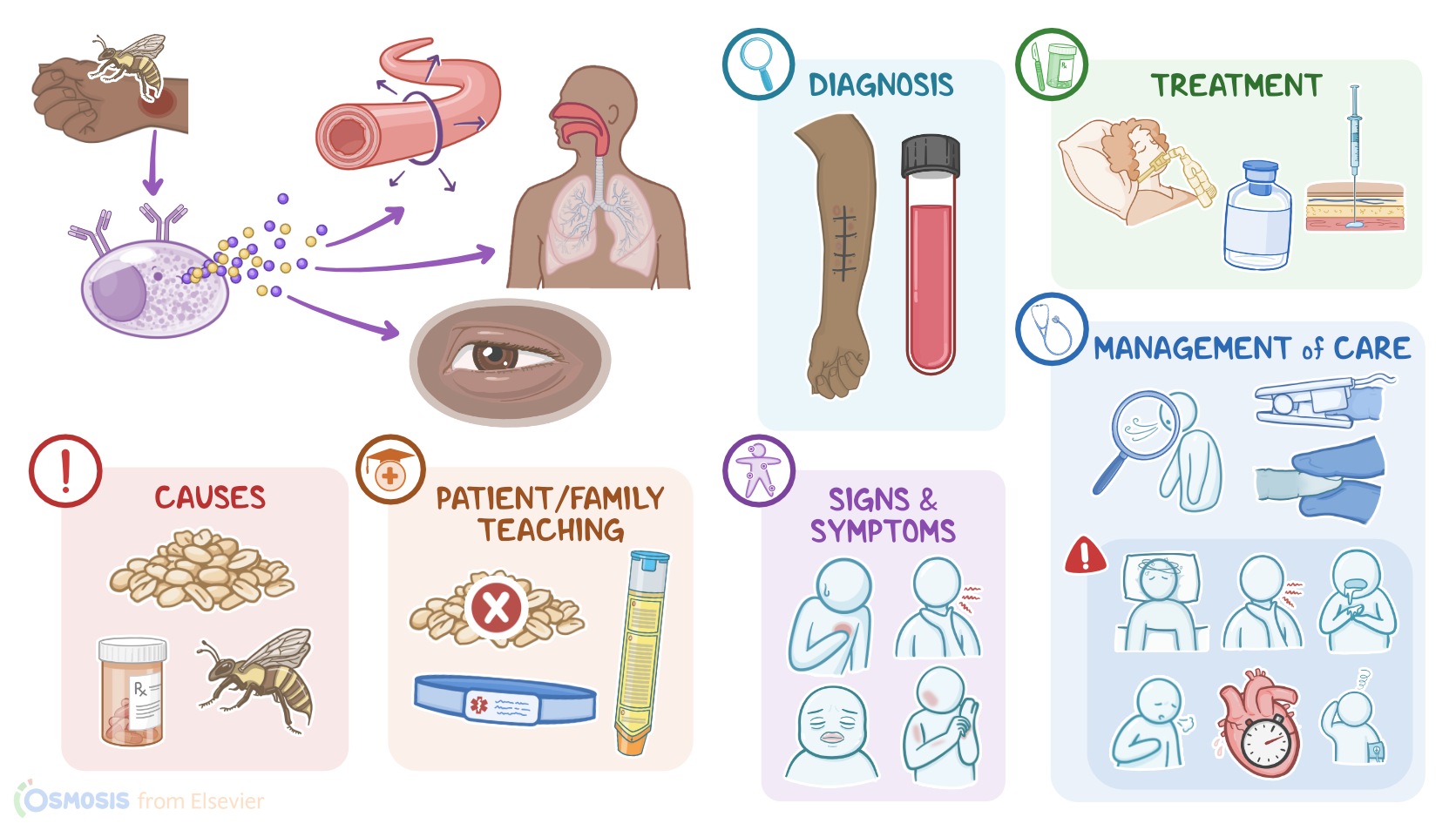
So, vasodilation, when blood volume is constant, lowers the blood pressure and slows down the blood flow through the blood vessels.Okay, now the main cause of anaphylaxis and anaphylactic shock is a systemic allergic reaction to an external trigger, which can be medications, insect bites, or food, for example, nuts. Important risk factors include certain comorbidities such as older age, asthma and other respiratory disorders like chronic obstructive pulmonary disease; or cardiovascular disease.
Now, let’s talk about pathology. The pathophysiologic mechanism behind anaphylaxis and anaphylactic shock is a type I hypersensitivity reaction, which is mediated by IgE antibodies that bind and sensitize the mast cells and basophils. Once an external trigger reaches the body, it binds IgE antibodies and stimulates mast cells and basophils to degranulate and release vasoactive mediators, such as histamine and bradykinin that eventually cause massive systemic vasodilation. Histamine also increases vascular permeability, thereby allowing the fluid to shift from the intravascular compartment into the interstitial compartment, subsequently causing edema. In addition to histamine, mast cells also release an enzyme tryptase, which breaks down the proteins and causes local tissue damage.
Now, the next events in anaphylactic shock are grouped into four stages: initial, compensatory, progressive, and refractory stages. In the initial stage, systemic vasodilation causes less blood to return to the heart through the venous system; this, in turn, decreases cardiac output. As a consequence, body cells are not well-perfused, so they switch to anaerobic metabolism to produce energy, causing lactic acid to build up in the blood. When lactic acid builds up, that lowers blood pH, causing metabolic acidosis. This activates the compensatory stage. During the compensatory stage, the sympathetic nervous system increases its activity to compensate for the decreased tissue perfusion in order to maintain homeostasis, and acid-base compensatory mechanisms activate to correct the acidosis. In the progressive stage, these compensatory mechanisms start failing, so the body’s metabolic needs can’t be met.
This results in lactic acid buildup in the blood, more than in the initial stage, and gradually worsening metabolic acidosis. Finally, the refractory stage is when shock progresses to cellular death and multiple organ damage, which can be fatal. Now, switching gears and moving on to complications. Reduced blood supply to the myocardium can result in myocardial infarction, while reduced blood supply to the brain might cause loss of consciousness. Additionally, the edema can affect the airway, more specifically, the larynx, and cause upper airway obstruction, respiratory failure, as well as complications, such as cardiorespiratory arrest and even death.