Spinal cord injury (SCI): Nursing
Notes
| SPINAL CORD INJURY (SCI) | ||
| KEY POINTS | NOTES | |
| DEFINITION |
| |
| PHYSIOLOGY |
| |
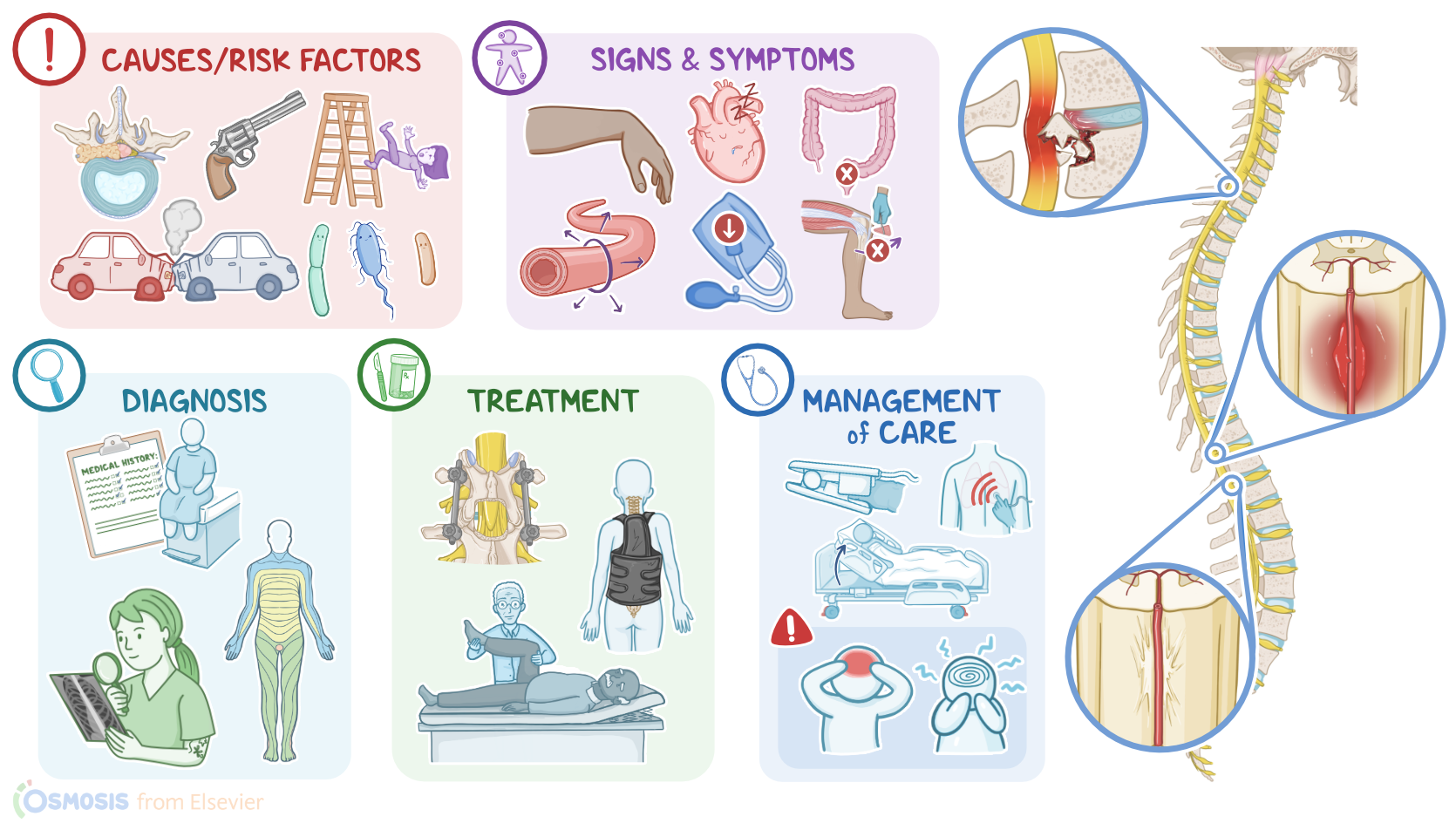
| CAUSES AND RISK FACTORS |
| |
| PATHOPHYSIOLOGY |
| |
| SIGNS AND SYMPTOMS |
| |
| DIAGNOSIS |
| |
| TREATMENT |
| |
| MANAGEMENT OF CARE |
| |
| PATIENT AND FAMILY TEACHING |
| |
Transcript
A spinal cord injury refers to any damage to the spinal cord, or the bundle of nerves protruding from the bottom of the spinal cord, called cauda equina. Now, let’s quickly review some anatomy and physiology. The spinal column consists of 33 vertebrae organized in 5 main regions: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 5 coccygeal. Together, the vertebrae create a bony canal that houses the spinal cord and surrounding meninges. The spinal cord is a bundle of nerve fibers that serves as a highway for information to travel between the brain and the rest of the body. This information is transmitted by highly specialized spinal tracts that carry motor information down the spinal cord to the body, and sensory information from the body up to the brain. The spinal cord travels through the spinal canal, and stops at the second lumbar vertebra. Here it ends in a cone, called conus medullaris. Since the spinal cord is shorter than the spinal canal, the nerves of the lumbar, sacral and coccygeal regions have to travel down the spinal canal to reach their corresponding openings. In doing so, they form a nerve bundle below the spinal cord called the cauda equina. Now, spinal cord injuries can have a number of different causes. In younger clients, most spinal cord injuries are caused by a motor vehicle crash; penetrating trauma, like a gunshot or a stab wound in the back; or recreational injuries, like those caused by impact sports or diving in shallow waters.
In older clients, though, spinal cord injuries are most often caused by severe falls, such as falling from a ladder; as well as medical conditions, including large tumors, infections, or degenerative diseases of the spine, like a protruding intervertebral disk or osteophytes. Risk factors for developing a spinal cord injury include engaging in high-risk behaviors, such as not wearing safety equipment when playing sports, speeding, and diving in shallow waters. Lastly, clients with a history of bone or joint disorders are also at a higher risk, since even minor trauma could damage the weakened bones, thereby injuring the spinal cord. Okay, so the pathology of a spinal cord injury can be primary and secondary. Primary injury typically involves a sudden, traumatic impact on the spine that fractures or dislocates vertebrae, causing compression on the spinal cord. After the primary injury, there is usually additional damage that occurs over the following days or weeks because of the body’s natural response to trauma, which is known as the secondary injury. The acute phase of the secondary injury begins immediately after the spinal injury, and includes bleeding, ischemia, and swelling on the site of the injury. As time goes by, there can be additional neuronal cell death caused by oxidative stress, neurotransmitter accumulation, and demyelination of surviving axons. Eventually, specialized glial cells begin to form a scar at the site of injury, which creates a barrier across the injured tissue that prevents the spread of neuronal damage. Unfortunately, since neurons have limited regenerative capacity, these injuries tend to yield permanent damage to the spinal cord.
All right, now clinical manifestations of spinal cord injuries depend on the severity and location of the injury, and may include partial or complete loss of sensation and motor function below the level of injury. Upper cervical lesions lead to quadriplegia, so there is loss of function of the limbs or trunk, and a ventilator is needed to maintain respiration. On the other hand, lower cervical lesions can still lead to a complete loss of trunk and lower limb function, however, some movements of the upper limb may remain intact, allowing for functions such as feeding or using a wheelchair. Next, thoracic lesions can also lead to paraplegia, where there’s paralysis of both lower limbs, but upper limb function remains intact. Thoracic lesions from T1 to T12, and lower cervical injury at C5 to C7, can impair intercostal muscle function, leading to shallow, ineffective breathing and impaired coughing. Lower thoracic and lumbar lesions can lead to some level of dysfunction of the lower limbs, resulting in difficulties with walking and ambulation. Finally, if the injury affects the nerves of the cauda equina, there may be decreased bowel and bladder control, as well as sexual dysfunction. It can also cause saddle anesthesia, which is a loss of sensation in the saddle area, which includes the buttocks, inner surface of the thigh, and perineum. Moreover, severe spinal cord injuries may result in spinal shock, which is a transient condition that develops shortly after an acute injury. It is characterized by flaccid paralysis, loss of sensation, and loss of deep tendon and sphincter reflexes below the level of injury. Neurogenic shock can also occur where the sympathetic neurons are damaged, leading to unopposed parasympathetic activity. This can cause peripheral vasodilation, hypotension, and bradycardia.
Diagnosis of a spinal cord injury starts with the client’s history and physical assessment. Next assess the severity of the injury by testing muscle function, as well as testing of sharp and dull sensation, and proprioception at each dermatome level. Then it’s scored using the American Spinal Injury Association or ASIA scale. The scale ranges from class A for a complete cord injury to E for normal nervous function. In addition, imaging tests like X-rays, CT scan, or MRI can be used to look for the exact cause of spinal cord injury. Treatment for spinal cord injuries begins with supportive measures to stabilize the client. This may include immobilizing the spinal column until an imaging test can be performed, as well as using ventilatory and cardiovascular support, if needed. After stabilization, treatment of spinal cord injuries is aimed at addressing the underlying cause, when possible. This may involve performing surgery to relieve any pressure from the spinal cord, known as decompression surgery, as well as stabilizing the spine to protect the spinal cord from further damage. Some clients may also receive corticosteroids to help reduce the inflammation. After the acute phase, much of the treatment is geared towards rehabilitation, which may involve optimal pain management, along with physical and occupational therapy. Finally, the goal of long-term care is to prevent and treat complications, as well as promote the client’s functional independence.
All right, now let’s look at the nursing care you will be providing for a client with a spinal cord injury. Your priority nursing goals are to assist in preventing complications and providing emotional support. First, work with the healthcare team to prevent complications by preventing further injury to your client’s spine. Apply a cervical collar to immobilize the neck, and keep their head in a neutral position. When repositioning your client, ask additional colleagues to help you move your client’s body as a unit using the log-roll technique. Then, support your client’s respiratory function by initiating high flow oxygen and continuous pulse oximetry. Assess their lung sounds as well as their respiratory rate and depth. Report to health care provider immediately any signs of respiratory dysfunction; including ineffective cough, SpO2 less than 93%, diminished lung sounds, or crackles, and tachypnea. Prepare to assist in intubation and mechanical ventilation, as indicated. Be sure to closely monitor their vital signs and watch for signs of neurogenic shock. Report bradycardia, hypotension, and warm, flush skin in the lower extremities. Administer the prescribed IV fluids and vasopressor medication, and atropine for symptomatic bradycardia. When your client is stable, prepare them for decompression and stabilization. Now, watch for signs of autonomic dysreflexia which is another significant complication. Report anxiety, headache, nasal stuffiness, bradycardia, and paradoxical hypertension, as well as coolness below the level of injury, and diaphoresis and flushing above the level of injury.